

Comparative analysis of hyperfibrinolysis with activated coagulation between amniotic fluid embolism and severe placental abruption
- PMID: 38168649
- PMCID: PMC10761968
- DOI: 10.1038/s41598-023-50911-w
Comparative analysis of hyperfibrinolysis with activated coagulation between amniotic fluid embolism and severe placental abruption
Abstract
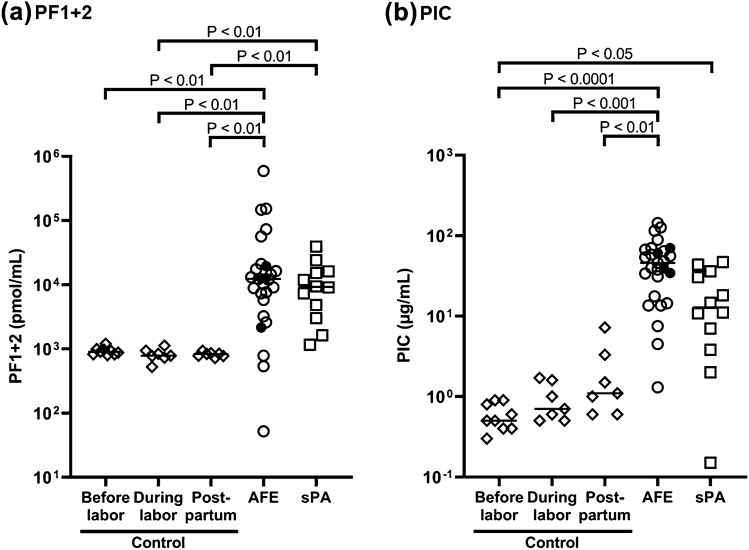
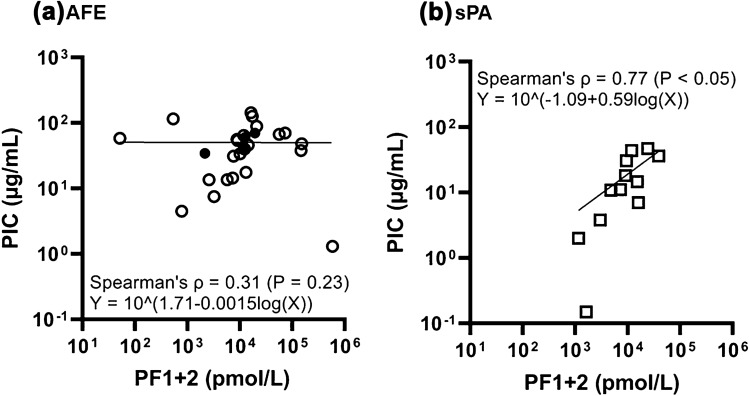
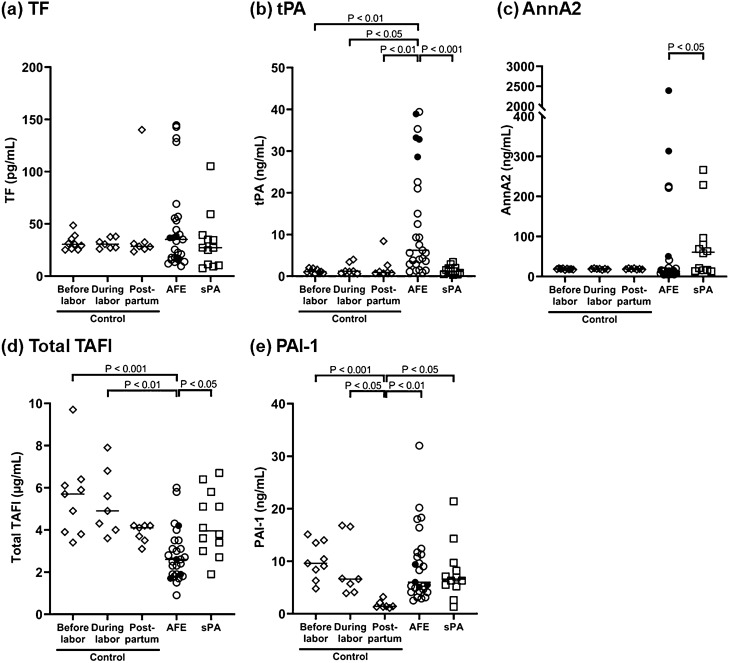
Amniotic fluid embolism (AFE) and placental abruption (PA) are typical obstetric diseases associated with disseminated intravascular coagulation (DIC). AFE is more likely to be complicated with enhanced fibrinolysis than PA. AFE may have an additional mechanism activating fibrinolytic cascade. We aimed to compare the coagulation/fibrinolysis factors among AFE, PA, and peripartum controls. We assessed AFE cases registered in the Japanese AFE Registry, and PA cases complicated with DIC (severe PA) and peripartum controls recruited at our hospital. The following factors in plasma were compared: prothrombin fragment 1 + 2 (PF1 + 2), plasmin α2-plasmin inhibitor complex (PIC), tissue factor (TF), tissue plasminogen activator (tPA), annexin A2 (AnnA2), total thrombin activatable fibrinolysis inhibitor (TAFI) including its activated form (TAFIa), and plasminogen activator inhibitor-type 1 (PAI-1). PF1 + 2 and PIC were markedly increased in both AFE (n = 27) and severe PA (n = 12) compared to controls (n = 23), without significant difference between those disease groups; however, PIC in AFE showed a tendency to elevate relative to PF1 + 2, compared with severe PA. AFE had significantly increased tPA and decreased total TAFI levels compared with severe PA and controls, which might be associated with further plasmin production in AFE and underlie its specific fibrinolytic activation pathway.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Page EW, King EB, Merrill JA. Abruptio placentae; dangers of delay in delivery. Obstet. Gynecol. 1954;3:385–393. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
