

The Ability of a 3-Gene Host Signature in Blood to Distinguish Tuberculous Meningitis From Other Brain Infections
- PMID: 38169323
- PMCID: PMC11326836
- DOI: 10.1093/infdis/jiad606
The Ability of a 3-Gene Host Signature in Blood to Distinguish Tuberculous Meningitis From Other Brain Infections
Abstract
Background: Tuberculous meningitis (TBM) is difficult to diagnose. We investigated whether a 3-gene host response signature in blood can distinguish TBM from other brain infections.
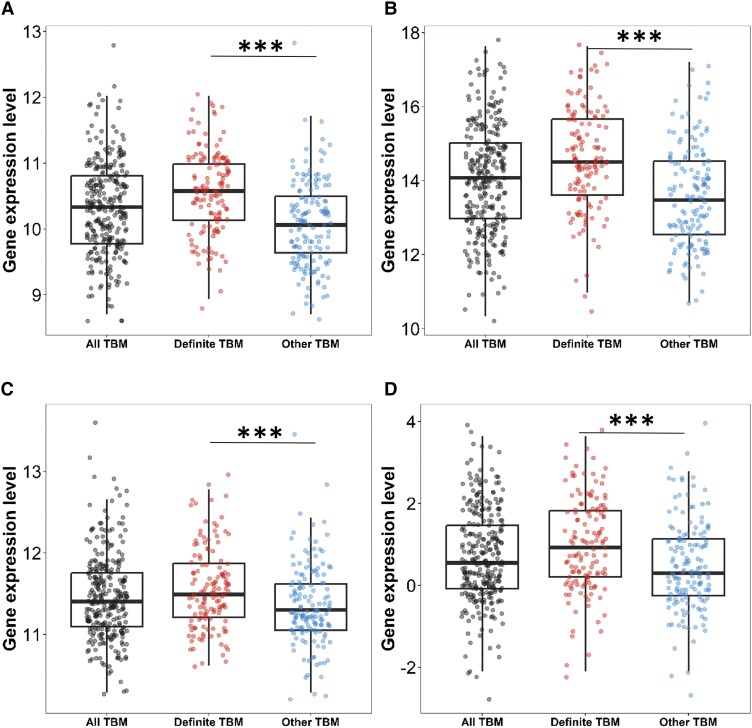
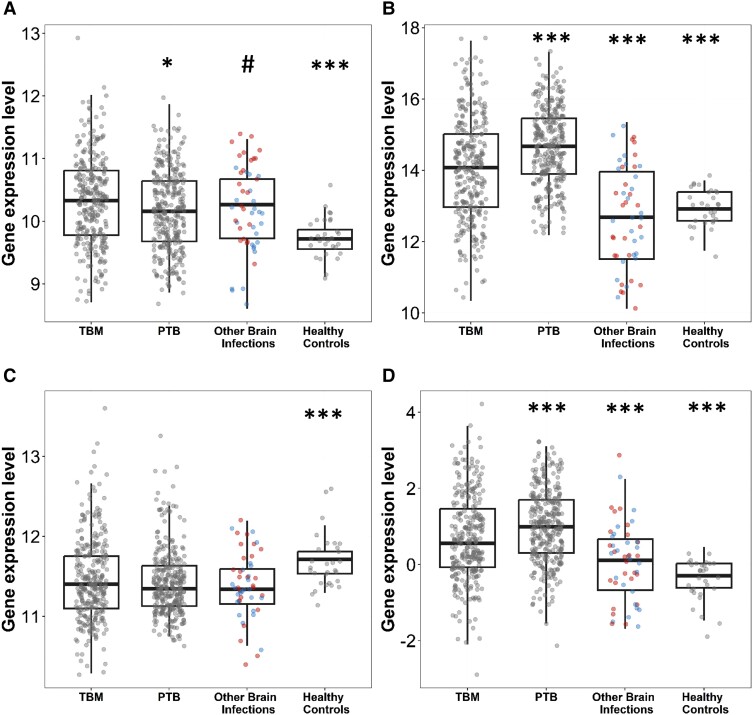
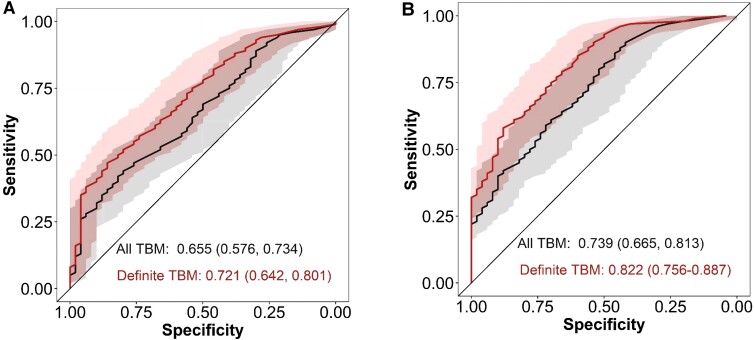
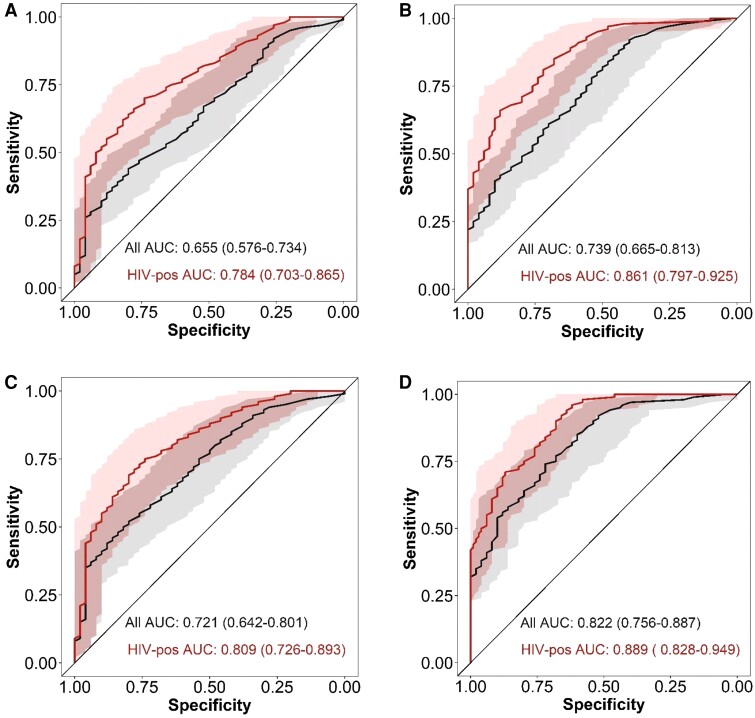
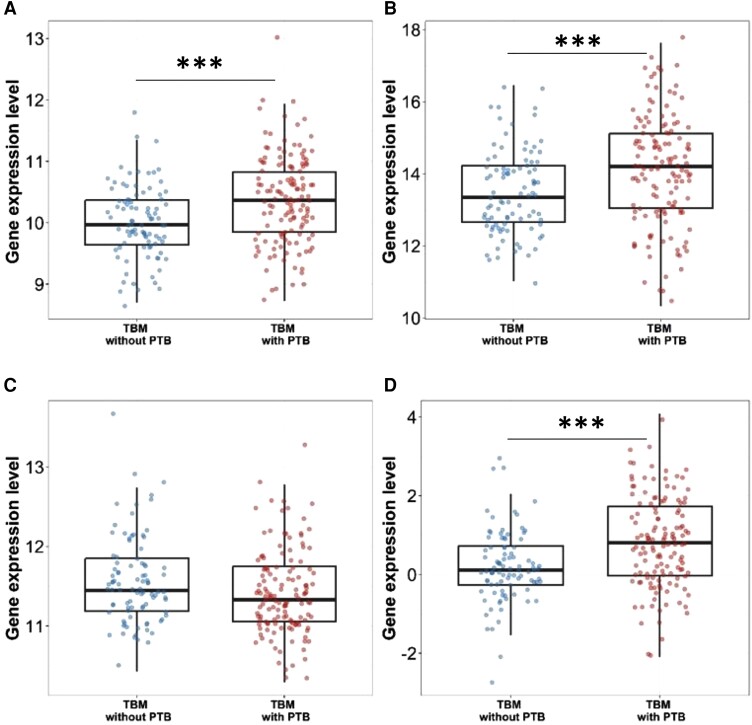
Methods: The expression of 3 genes (dual specificity phosphatase 3 [DUSP3], guanylate-binding protein [GBP5], krupple-like factor 2 [KLF2]) was analyzed by RNA sequencing of archived whole blood from 4 cohorts of Vietnamese adults: 281 with TBM, 279 with pulmonary tuberculosis, 50 with other brain infections, and 30 healthy controls. Tuberculosis scores (combined 3-gene expression) were calculated following published methodology and discriminatory performance compared using area under a receiver operator characteristic curve (AUC).
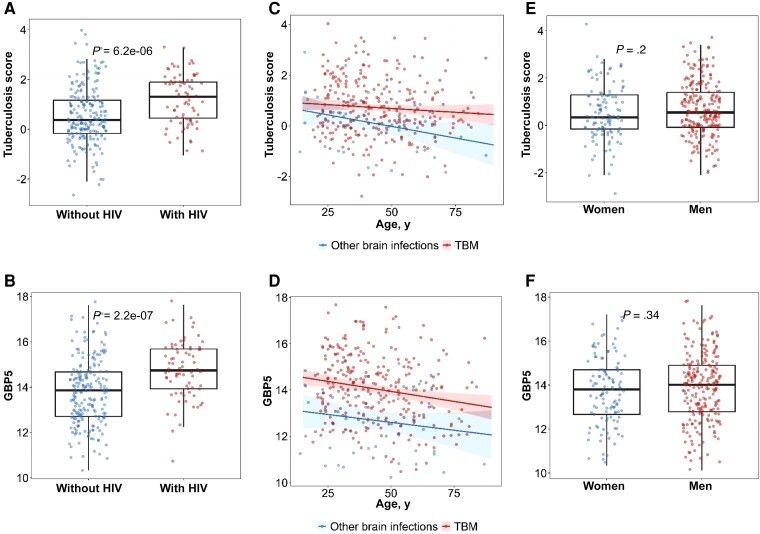
Results: GBP5 was upregulated in TBM compared to other brain infections (P < .001), with no difference in DUSP3 and KLF2 expression. The diagnostic performance of GBP5 alone (AUC, 0.74; 95% confidence interval [CI], .67-.81) was slightly better than the 3-gene tuberculosis score (AUC, 0.66; 95% CI, .58-.73) in TBM. Both GBP5 expression and tuberculosis score were higher in participants with human immunodeficiency virus (HIV; P < .001), with good diagnostic performance of GBP5 alone (AUC, 0.86; 95% CI, .80-.93).
Conclusions: The 3-gene host signature in whole blood has the ability to discriminate TBM from other brain infections, including in individuals with HIV. Validation in large prospective diagnostic study is now required.
Keywords: 3-gene host response; HIV coinfection; brain infections; diagnosis; tuberculous meningitis.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. All authors: No reported conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- World Health Organization . Global tuberculosis report 2022. Geneva, Switzerland: WHO, 2022.
-
- Chiang S, Khan F, Milstein M, et al. . Treatment outcomes of childhood tuberculous meningitis: a systematic review and meta-analysis. Lancet Infect Dis 2014; 14:947–57. - PubMed
-
- Thwaites GE, Tran TH. Tuberculous meningitis: many questions, too few answers. Lancet Neurol 2005; 4:160–70. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
