

Contingent negative variation as an evaluation indicator of neurocognitive disorder after traumatic brain injury
- PMID: 38169851
- PMCID: PMC10758395
- DOI: 10.3389/fpsyt.2023.1255608
Contingent negative variation as an evaluation indicator of neurocognitive disorder after traumatic brain injury
Abstract
Introduction: Neurocognitive disorders are commonly observed in patients suffering from traumatic brain injury (TBI). Methods to assess neurocognitive disorders have thus drawn the general attention of the public, especially electrophysiology parameter such as contingent negative variation (CNV), which has been given more emphasis as a neurophysiological marker in event-related potentials (ERPs) for diagnosing a neurocognitive disorder and assessing its severity. The present study focused on the correlations between CNV parameters and levels of daily living activities and social function to explore the potential of CNV as an objective assessment tool.
Methods: Thirty-one patients with a diagnosis of neurocognitive disorder after a TBI according to ICD-10 were enrolled as the patient group, and 24 matched healthy volunteers were enrolled as the control group. The activity of daily living scale, functional activities questionnaire, social disability screening schedule, and scale of personality change following TBI were used to assess daily living activity and social function.
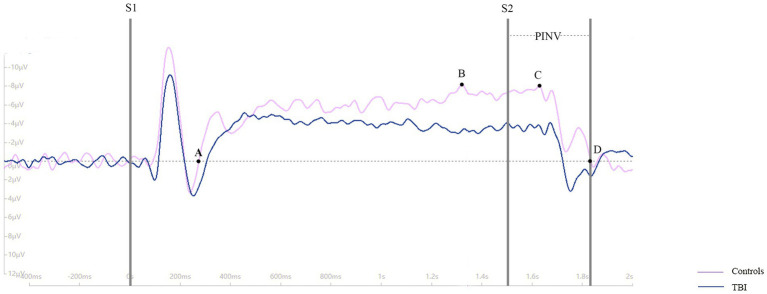
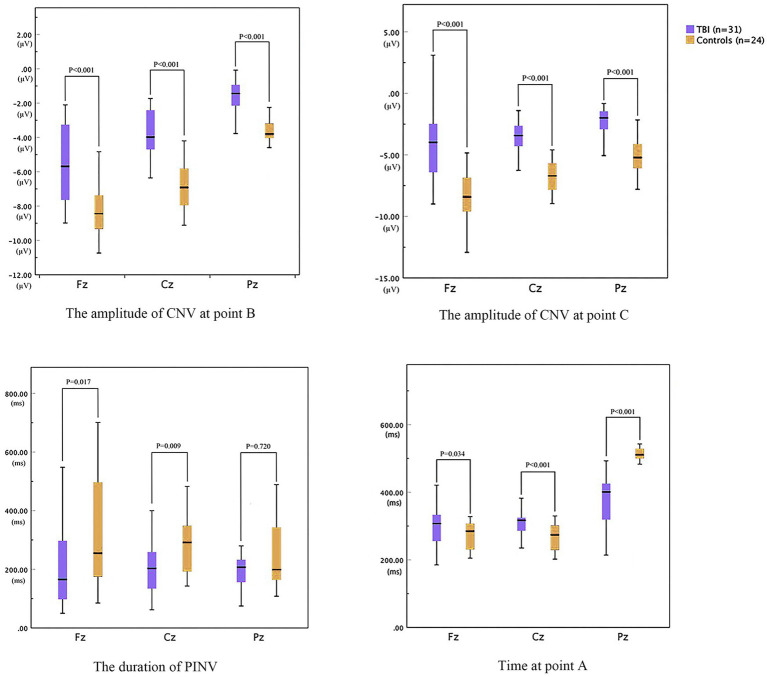
Results: The scale scores in patients were significantly higher than those in controls. Maximum amplitudes before S2 and during the post-imperative negative variation (PINV) period were also significantly higher in the patient group compared to the control group and were positively correlated with four scale scores. The duration of PINV at Fz and Cz was significantly shorter in the patient group than in the control group. The CNV return to baseline from a positive wave at electrode Fz and Cz occurred significantly earlier in the control group than in the patient group, while at Pz, the result showed the opposite.
Conclusion: Lower amplitudes of CNV were associated with more severe neurocognitive disorder and greater impairments in daily life abilities and social function. The duration of PINV and the latency of returning to baseline from a positive wave were correlated with the neurocognitive disorder to some extent. CNV could be used as an objective, electrophysiology-based parameter for evaluating the severity of the neurocognitive disorder and personality changes after TBI.
Keywords: contingent negative variation; evaluation indicator; event-related potential; neurocognitive disorder; traumatic brain injury.
Copyright © 2023 Ling, Wang, Zhang, Li, Zhang, Cai and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
P300 as a Potential Indicator in the Evaluation of Neurocognitive Disorders After Traumatic Brain Injury.Front Neurol. 2021 Sep 9;12:690792. doi: 10.3389/fneur.2021.690792. eCollection 2021. Front Neurol. 2021. PMID: 34566838 Free PMC article.
-
Application of Mismatch Negative in Evaluation of Severity of Mental Disorders due to Traumatic Brain Injury.Fa Yi Xue Za Zhi. 2019 Dec;35(6):695-700. doi: 10.12116/j.issn.1004-5619.2019.06.009. Epub 2019 Dec 25. Fa Yi Xue Za Zhi. 2019. PMID: 31970956 Chinese, English.
-
Contingent negative variation in patients with deficit schizophrenia or bipolar I disorder with psychotic features: measurement and correlation with clinical characteristics.Nord J Psychiatry. 2015 Apr;69(3):196-203. doi: 10.3109/08039488.2014.959562. Epub 2014 Sep 29. Nord J Psychiatry. 2015. PMID: 25263850
-
Permanent or transitory effects on neurocognitive components of the CNV complex induced by brain dysfunctions, lesions and ablations in humans.Int J Psychophysiol. 2003 May;48(2):189-220. doi: 10.1016/s0167-8760(03)00054-0. Int J Psychophysiol. 2003. PMID: 12763574 Review.
-
Brain electrical activity (quantitative EEG and bit-mapping neurocognitive CNV components), psychometrics and clinical findings in presenile subjects with initial mild cognitive decline or probable Alzheimer-type dementia.Ital J Neurol Sci. 1995 Sep;16(6):341-76. doi: 10.1007/BF02229172. Ital J Neurol Sci. 1995. PMID: 8626214 Review.
References
-
- Gudigar A, Raghavendra U, Hegde A, Menon GR, Molinari F, Ciaccio EJ, et al. . Automated detection and screening of traumatic brain injury (Tbi) using computed tomography images: a comprehensive review and future perspectives. Int J Environ Res Public Health. (2021) 18:6499. doi: 10.3390/ijerph18126499, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources