

Optimization of lung ultrasound in ultrafast-track anesthesia for non-cyanotic congenital heart disease surgery
- PMID: 38169938
- PMCID: PMC10758866
- DOI: 10.1016/j.heliyon.2023.e23544
Optimization of lung ultrasound in ultrafast-track anesthesia for non-cyanotic congenital heart disease surgery
Abstract
Objective: We aimed to explore the feasibility of lung ultrasound for perioperative assessment and the optimal effect of lung ultrasound in reducing lung complications during non-cyanotic congenital heart disease (CHD) surgery using ultrafast-track anesthesia.
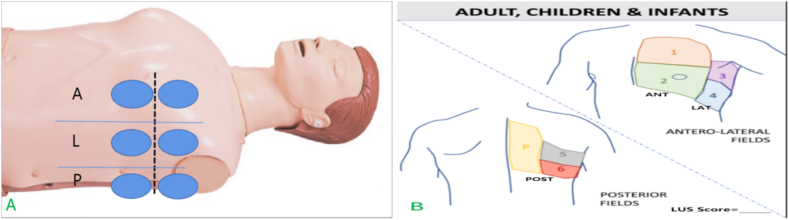
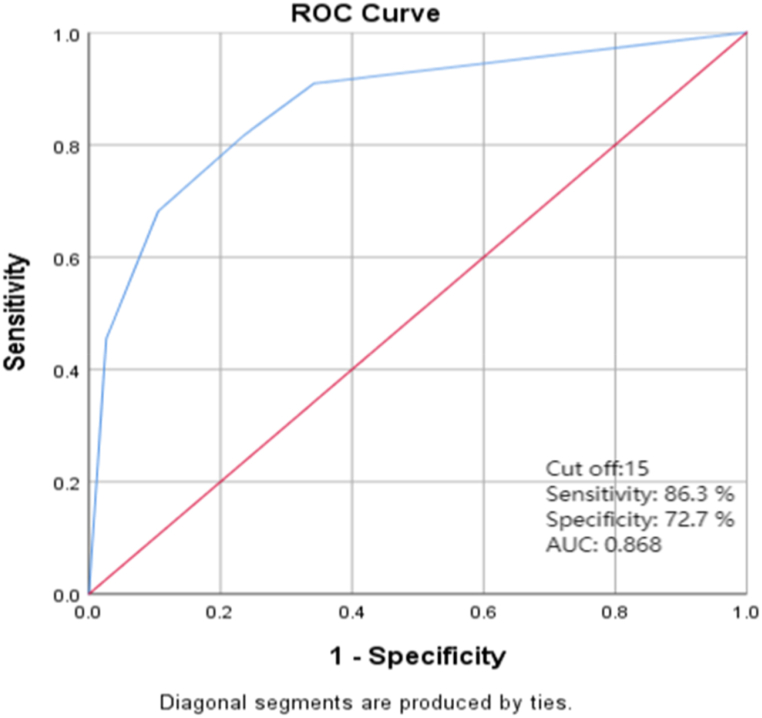
Methods: Sixty patients were treated at Shenzhen Children's Hospital between 2019 and 2020. Of these, 30 patients in group N had an indication for extubation and ultrafast-track anesthesia after congenital heart surgery; the tracheal catheter was removed, and the patients were sent to the cardiac intensive care unit (CICU) for further monitoring and treatment. Another 30 patients were in group L and also had an indication for extubation and ultrafast-track anesthesia; in addition we compared lung ultrasound score (LUS) before and after surgery, when we found the cases that LUS ≥ 15, for whom targeted optimization treatment would be carried out. The tracheal catheter was removed after LUS <15 days before the patients were sent to the CICU. In all cases, the LUS and PaO2/FiO2 ratios (P/F) of both groups were recorded at the time of anesthesia induction (T0), before extubation (T1), and 5 min (T2), 1 h (T3), and 24 h (T4) after extubation. The incidence of pulmonary complications, LUS, and P/F were compared between the two groups.
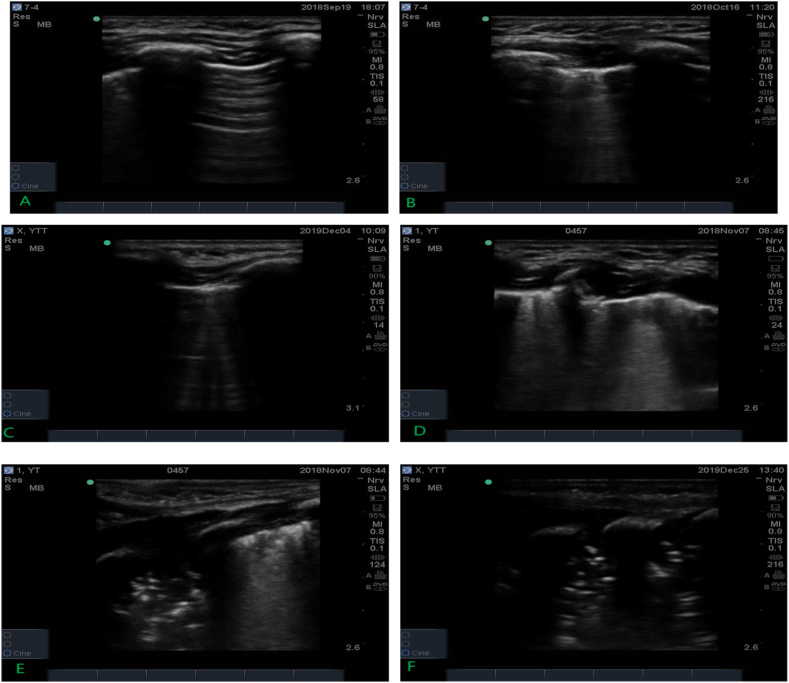
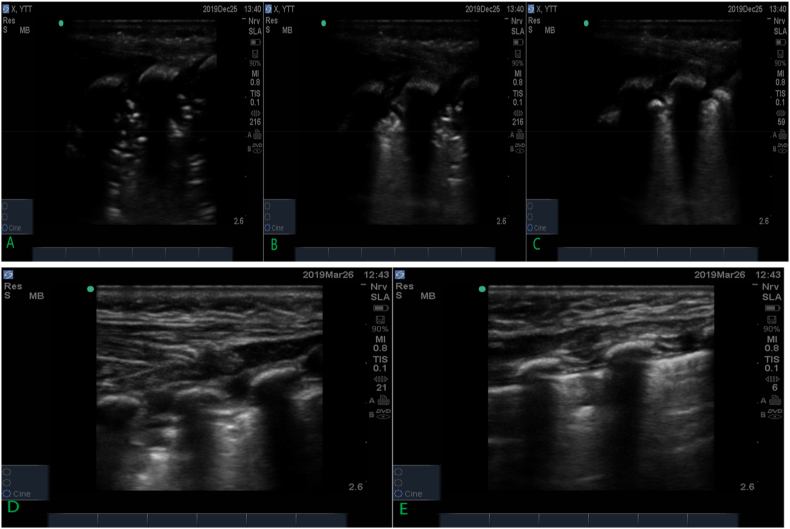
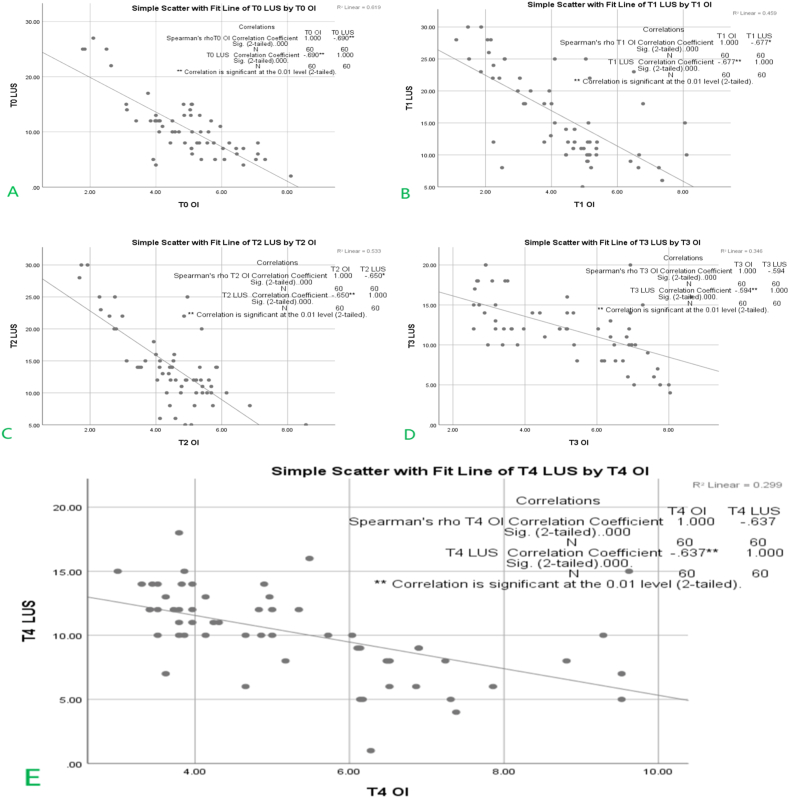
Results: There was great consistency between LUS and radiographic findings. Comparing the data of the two groups at T2, T3 and T4, the P/F was higher and the LUS was lower in group L than in group N. The incidence of lung complications in group L (18 cases, 60 %) was lower than that in group N (26 cases, 86.7 %, χ2 = 5.46, P = 0.02); comparing LUS between T0 and T3, LUS decreased in a greater number of cases in group L (15, 50 %) than in group N (7 cases, 23.3 %, χ2 = 4.59, P = 0.032).
Conclusion: Lung ultrasonography can effectively help assess lung conditions. Optimization guided by lung ultrasound in ultrafast track anesthesia can significantly reduce postoperative lung complications.
Keywords: Lung ultrasound; Non-cyanotic congenital heart disease; Optimization; Ultrafast-track anesthesia.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
The Effects of a Pre-Extubation Single Recruitment Maneuver on Ultrasonographic Lung Conditions in Patients Undergoing Lateral Decubitus Surgery: A Randomized Clinical Trial.J Clin Med. 2025 Apr 25;14(9):2969. doi: 10.3390/jcm14092969. J Clin Med. 2025. PMID: 40364000 Free PMC article.
-
Effect of recruitment manoeuvres under lung ultrasound-guidance and positive end-expiratory pressure on postoperative atelectasis and hypoxemia in major open upper abdominal surgery: A randomized controlled trial.Heliyon. 2023 Jan 30;9(2):e13348. doi: 10.1016/j.heliyon.2023.e13348. eCollection 2023 Feb. Heliyon. 2023. PMID: 36755592 Free PMC article.
-
Evaluation of perioperative lung ultrasound scores in robotic radical prostatectomy: prospective observational study.J Robot Surg. 2025 Mar 11;19(1):112. doi: 10.1007/s11701-025-02272-x. J Robot Surg. 2025. PMID: 40069409 Free PMC article.
-
Effects of small-dose S-ketamine on anesthesia-induced atelectasis in patients undergoing general anesthesia accessed by lung ultrasound: study protocol for a randomized, double-blinded controlled trial.Trials. 2024 Jan 18;25(1):64. doi: 10.1186/s13063-023-07779-y. Trials. 2024. PMID: 38238838 Free PMC article.
-
Lung ultrasound score in establishing the timing of intubation in COVID-19 interstitial pneumonia: A preliminary retrospective observational study.PLoS One. 2020 Sep 3;15(9):e0238679. doi: 10.1371/journal.pone.0238679. eCollection 2020. PLoS One. 2020. Retraction in: PLoS One. 2020 Dec 31;15(12):e0245032. doi: 10.1371/journal.pone.0245032. PMID: 32881950 Free PMC article. Retracted.
References
LinkOut - more resources
Full Text Sources
