Clinical Features of Autoimmune Nodopathy With Anti-Neurofascin-155 Antibodies in South Koreans
- PMID: 38171501
- PMCID: PMC10921045
- DOI: 10.3988/jcn.2023.0055
Clinical Features of Autoimmune Nodopathy With Anti-Neurofascin-155 Antibodies in South Koreans
Abstract
Background and purpose: Anti-neurofascin-155 (NF155) antibody is one of the autoantibodies associated with autoimmune nodopathy. We aimed to determine the clinical features of South Korean patients with anti-NF155-antibody-positive autoimmune nodopathy.
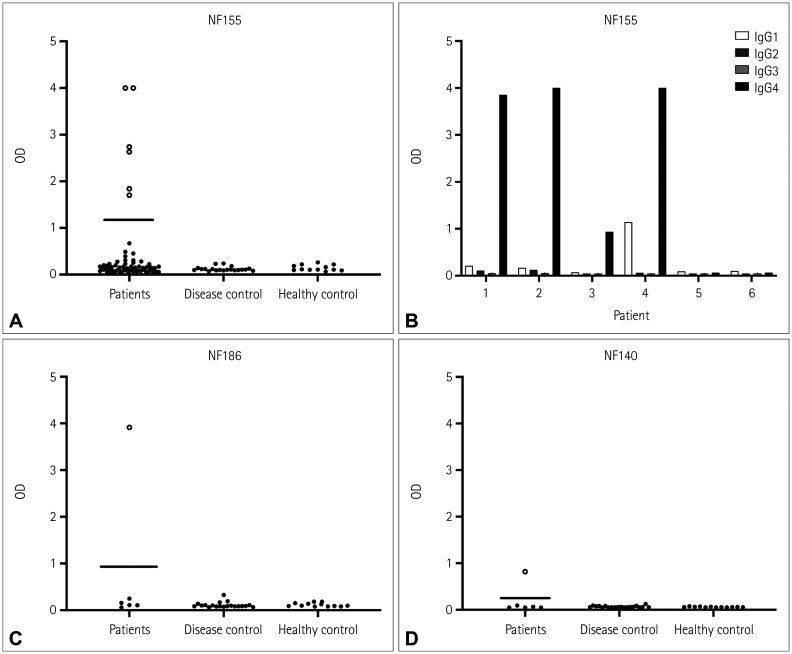
Methods: The sera of 68 patients who fulfilled the diagnostic criteria for chronic inflammatory demyelinating polyneuropathy (CIDP) were tested for anti-NF155 antibodies using a cell-based assay (CBA) and enzyme-linked immunosorbent assay (ELISA). The anti-NF155-positive sera were also assayed for NF155 immunoglobulin G (IgG) subclasses, and for anti-NF186 and NF140 antibodies. The clinical features of the patients were reviewed retrospectively.
Results: Among the 68 patients, 6 (8.8%) were positive for anti-NF155 antibodies in both the CBA and ELISA. One of those six patients was also positive for anti-NF186 and anti-NF140 antibodies. IgG4 was the predominant subclass in four patients. The mean age at onset was 32.2 years. All six positive patients presented with progressive sensory ataxia. Five patients treated using corticosteroids presented a partial or no response. All six patients were treated using intravenous immunoglobulin (IVIg). Among them, five exhibited a partial or poor response and the other exhibited a good response. All three patients treated using rituximab showed a good response.
Conclusions: The clinical characteristics of the patients were consistent with those in previous studies. Anti-NF155 antibody assay is necessary for diagnosing autoimmune nodopathy and its appropriate treatment, especially in young patients with CIDP who present with sensory ataxia and poor therapeutic responses to corticosteroids and IVIg.
Keywords: autoantibodies; autoimmune diseases; neurofascin; nodes of Ranvier; peripheral neuropathy.
Copyright © 2024 Korean Neurological Association.
Conflict of interest statement
Ha Young Shin, a contributing editor of the Journal of Clinical Neurology, was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Figures


References
-
- Querol L, Devaux J, Rojas-Garcia R, Illa I. Autoantibodies in chronic inflammatory neuropathies: diagnostic and therapeutic implications. Nat Rev Neurol. 2017;13:533–547. - PubMed
-
- Rasband MN, Peles E. Mechanisms of node of Ranvier assembly. Nat Rev Neurosci. 2021;22:7–20. - PubMed
-
- Van den Bergh PYK, van Doorn PA, Hadden RDM, Avau B, Vankrunkelsven P, Allen JA, et al. European Academy of Neurology/Peripheral Nerve Society guideline on diagnosis and treatment of chronic inflammatory demyelinating polyradiculoneuropathy: report of a joint task force-second revision. Eur J Neurol. 2021;28:3556–3583. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources