

Social and clinical vulnerability in stroke and STEMI management during the COVID-19 pandemic: a registry-based study
- PMID: 38171619
- PMCID: PMC10773394
- DOI: 10.1136/bmjopen-2023-073933
Social and clinical vulnerability in stroke and STEMI management during the COVID-19 pandemic: a registry-based study
Abstract
Objective: This study aims to evaluate whether the first wave of the COVID-19 pandemic resulted in a deterioration in the quality of care for socially and/or clinically vulnerable stroke and ST-segment elevation myocardial infarction (STEMI) patients.
Design: Two cohorts of STEMI and stroke patients in the Aquitaine neurocardiovascular registry.
Setting: Six emergency medical services, 30 emergency units, 14 hospitalisation units and 11 catheterisation laboratories in the Aquitaine region in France.
Participants: This study involved 9218 patients (6436 stroke and 2782 STEMI patients) in the neurocardiovascular registry from January 2019 to August 2020.
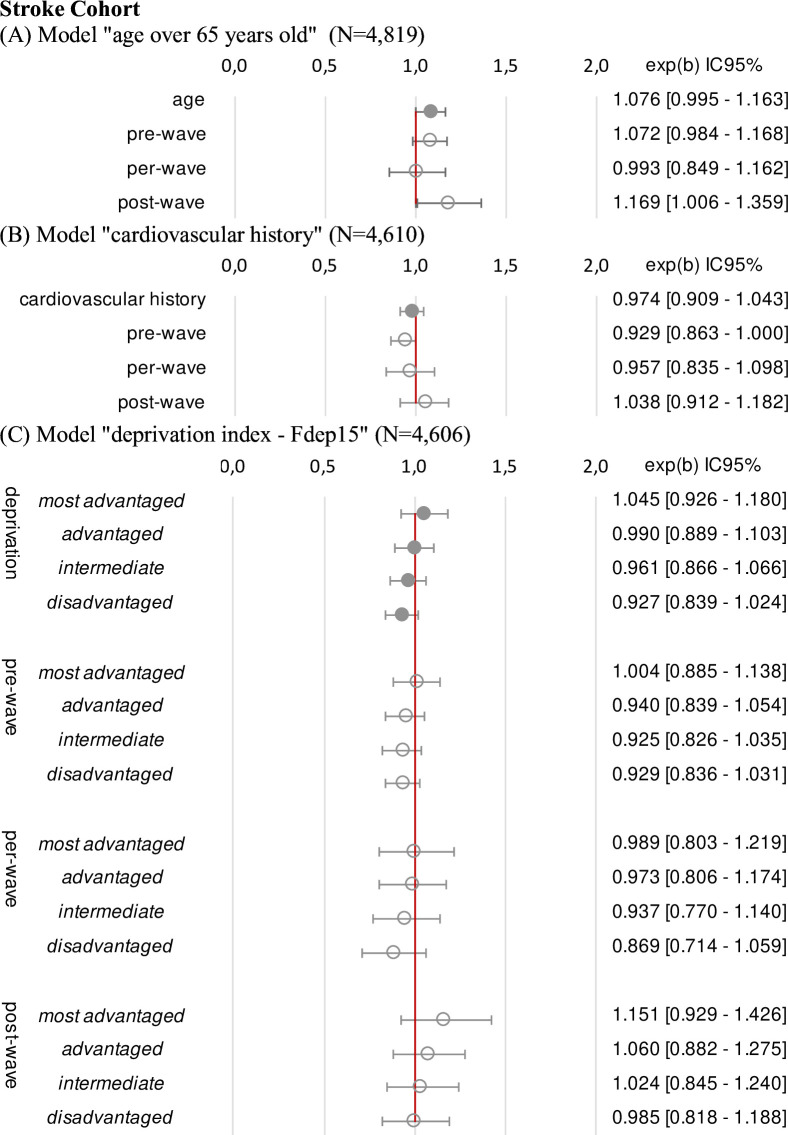
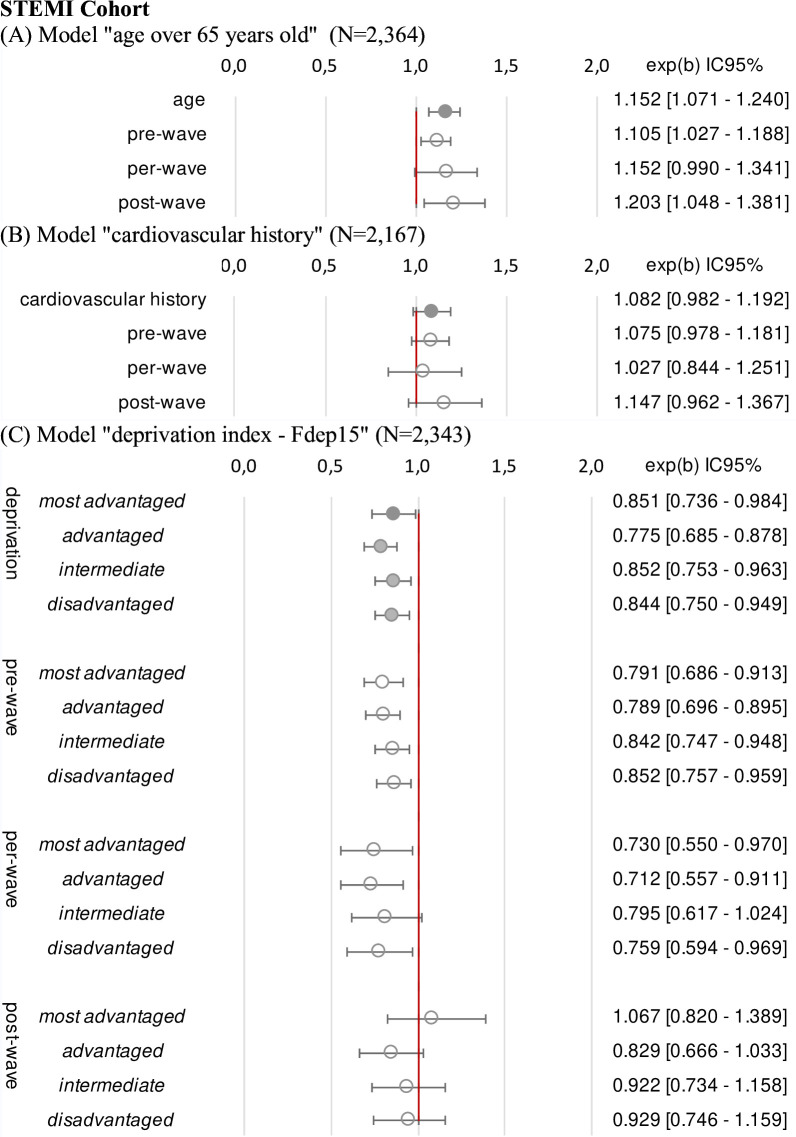
Primary outcome measures: Care management times in both cohorts: first medical contact-to-procedure time for the STEMI cohort and emergency unit admission-to-imaging time for the stroke cohort. Associations between social (deprivation index) and clinical (age >65 years, neurocardiovascular history) vulnerabilities and care management times were analysed using multivariate linear mixed models, with an interaction on the time period (pre-wave, per-wave and post-first COVID-19 wave).
Results: The first medical contact procedure time was longer for elderly (p<0.001) and 'very socially disadvantaged' (p=0.003) STEMI patients, with no interaction regarding the COVID-19 period (age, p=0.54; neurocardiovascular history, p=0.70; deprivation, p=0.64). We found no significant association between vulnerabilities and the admission imaging time for stroke patients, and no interaction with respect to the COVID-19 period (age, p=0.81; neurocardiovascular history, p=0.34; deprivation, p=0.95).
Conclusions: This study revealed pre-existing inequalities in care management times for vulnerable STEMI and stroke patients; however, these inequalities were neither accentuated nor reduced during the first COVID-19 wave. Measures implemented during the crisis did not alter the structured emergency pathway for these patients.
Trial registration number: NCT04979208.
Keywords: COVID-19; Health Equity; Health Services Accessibility; Health policy; Organisation of health services; Quality in health care.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical