

Features of acute COVID-19 associated with post-acute sequelae of SARS-CoV-2 phenotypes: results from the IMPACC study
- PMID: 38172101
- PMCID: PMC10764789
- DOI: 10.1038/s41467-023-44090-5
Features of acute COVID-19 associated with post-acute sequelae of SARS-CoV-2 phenotypes: results from the IMPACC study
Abstract
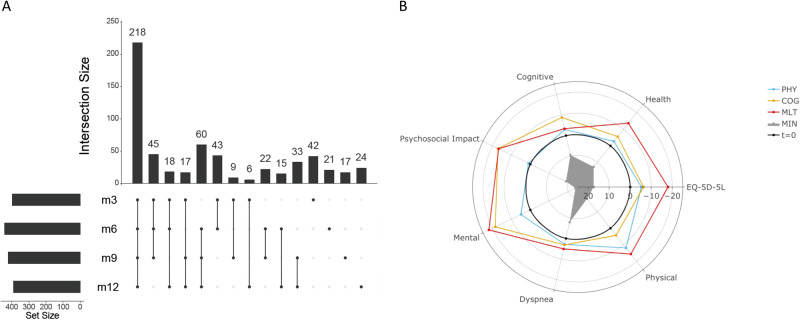
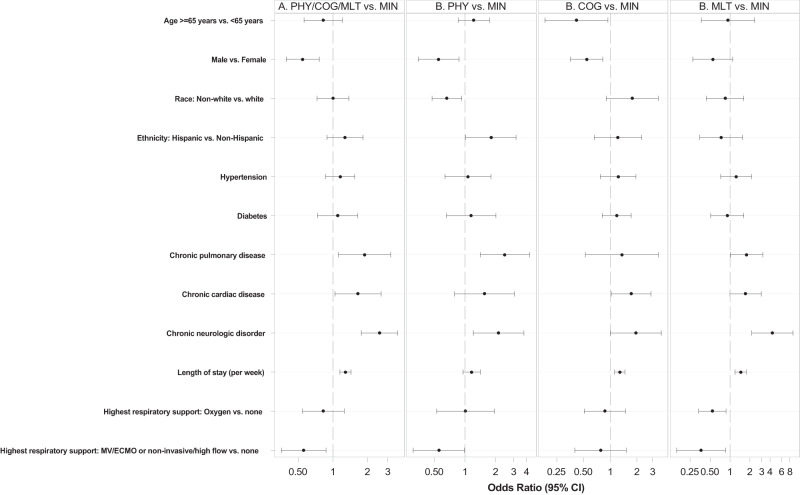
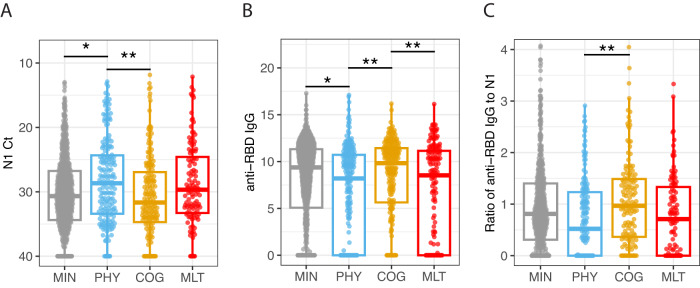
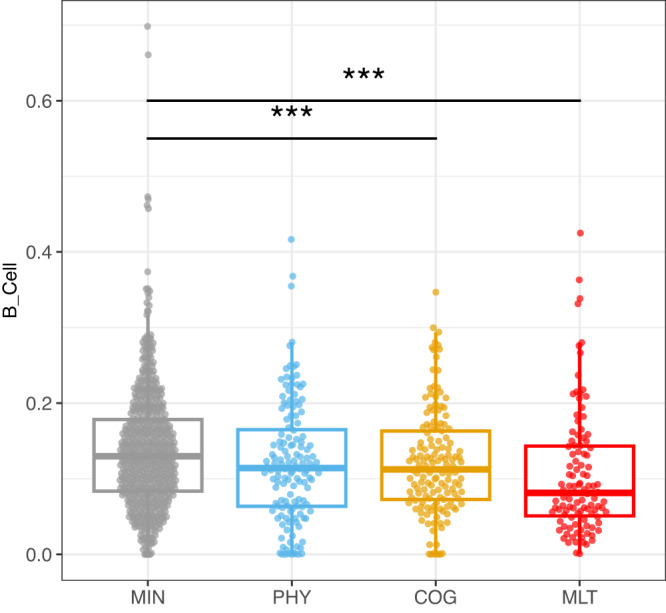
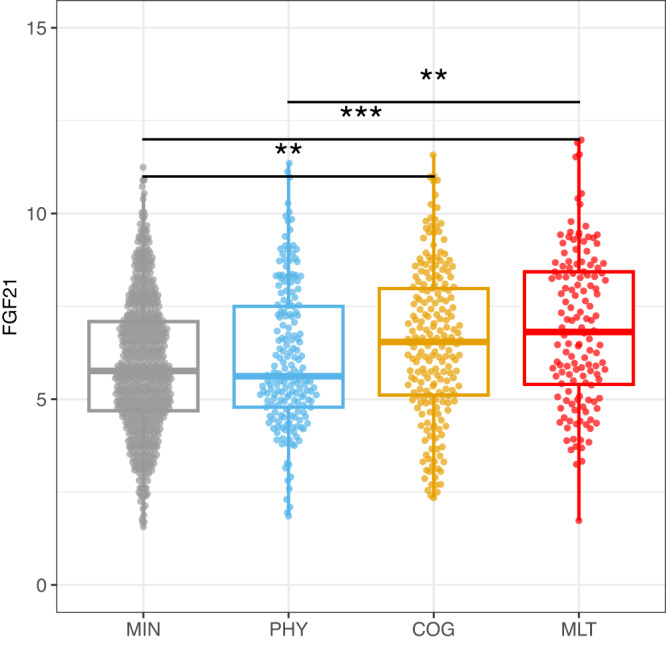
Post-acute sequelae of SARS-CoV-2 (PASC) is a significant public health concern. We describe Patient Reported Outcomes (PROs) on 590 participants prospectively assessed from hospital admission for COVID-19 through one year after discharge. Modeling identified 4 PRO clusters based on reported deficits (minimal, physical, mental/cognitive, and multidomain), supporting heterogenous clinical presentations in PASC, with sub-phenotypes associated with female sex and distinctive comorbidities. During the acute phase of disease, a higher respiratory SARS-CoV-2 viral burden and lower Receptor Binding Domain and Spike antibody titers were associated with both the physical predominant and the multidomain deficit clusters. A lower frequency of circulating B lymphocytes by mass cytometry (CyTOF) was observed in the multidomain deficit cluster. Circulating fibroblast growth factor 21 (FGF21) was significantly elevated in the mental/cognitive predominant and the multidomain clusters. Future efforts to link PASC to acute anti-viral host responses may help to better target treatment and prevention of PASC.
© 2024. The Author(s).
Conflict of interest statement
M.C.A. has received grant support from NIH-R01AI32774 for this project funded through this R01 and travel fees from NIAID for travel to the American Thoracic Society 2022 to present data related to this study. M.A.A. has received funding from NIH, NIAID-5U54AI142766-03 through institution. L.R.B. has received grant support from NIH NIAID, through institution. P.M.B. and A.D.A. federal employees serving as a project scientist for this project but had no role in funding decisions or oversight of relevant grants. B.P. has received funding from NIH/NIAID. C.B.C. has received funding from NIAID with payments to institution (Drexel University), Bill & Melinda Gates Foundation for COVID-19 work paid to institution, consulting fees from bioMerieux on clinical biomarkers, serves as DSMB, Advisory board for Convalescent Plasma COVID-19 study for the National Heart, Lung and Blood Institute (NHLBI), and is acting Leadership as President Board of Directors for the National Foundation of Emergency Medicine (NFEM), a non-profit supporting emergency medicine research and researchers. C.C. has received funding from NHLBI, grants from Bayer, Roche-Genentech, Quantum Leap Healthcare Collaborative, and consulting fees from Vasomune, Gen1e Life Sciences, Cellenkos, Janssen. L.E. has received grant funding from NIH R01AI104870-S1. D.E. has received NIH grants awarded to institution (UCSF). C.L.H. has received funding from NIH and the American Lung Association, travel support from Stanford, Harvard, Critical Care Clinical Trialists, Critical Care Reviews, and the University of Michigan, serves as DSMB Quantum Health for iSPY COVID, and paid participation as member, Board of Directors for American Thoracic Society. J.P.M. has received funding from NIH Grant # 3U19AI0626629-17S2. S.H.K. has received paid consulting fees from Peraton for personal consulting related to Immport data repository. M.K. has received grants support from NIAID through institution (University of Arizona). F.K.R. has received funding from NIAID Collaborative Influenza Vaccine Innovation Centers (CIVIC) contract 75N93019C00051, JPB Foundation and the Open Philanthropy Project (research grant 2020-215611, 5384), National Cancer Institute, NIH contract no.75N91019D00024, Task order no. 75N91020F00003, research funding from Pfizer for development of animal models for SARS-CoV-2, consulting fees from Pfizer, Seqirus, Avimex, Third Rock Ventures, paid lecture fees, and patents filed at the Icahn School of Medicine at Mount Sinai relating to SARS-CoV-2 serological assays (the “Serology Assays” and NDV-based SARS-CoV-2 vaccines which list F.K.R. as co-inventor). G.A.M. has received consulting fees from Gilead. E.M. has received funding from the NIH IMPACC R01AI104870-S1, grants from Babson Diagnostics, K0826-1616-11 through Institution Dell Medical School at UT Austin, paid speaker fees from MS Association of America, and serves as DSMB for Advisory boards of Genentech, Horizon, Teva and Viela Bio. W.B.M. has received funding from NIH NIAID R01AI14583. R.R.M. has contracts and grants for IMPACC study from NIAID AI 089992 aid and a Leadership Councilor role 2018-2021 for Society of Leukocyte Biology. K.C.N. has research funding from the National Heart, Lung, and Blood Institute (NHLBI), National Institute of Environmental Health Sciences (NIEHS), Food Allergy Research & Education (FARE), Director of the World Allergy Organization center of Excellence for Stanford and National Institute of Allergy and Infectious Diseases (NIAID) through institution, paid participation for service on Data Safety Monitoring Board of Director from World Allergy Organization Center of Excellence for Stanford, earns stocks as co-founder at Seed Health, IgGenix, ClostraBio, ImmuneID and financial interests as advisor and co-founder for Cour Pharma, Before Brands, Alladapt, and Latitude, is a national scientific committee member for Network ITN, NIH clinical research centers, and has listed Patents: Mixed allergen composition and methods for using the same Granulocyte-based methods for detecting and monitoring immune system disorders, licensee: (Alladapt and Before Brands no: US15/048,609); Application number: US12/610,94 Methods and Assays for Detecting and Quantifying Pure Subpopulations of White blood cells in immune system disorders. O.L. has received NIH/NIAID grants through institution for Human Immunology Project Consortium Funding (U19) 1-U19-AI118608-01A1 as PI Role and support as a speaker for presentation regarding the Coronavirus pandemic from Midsized Bank Coalition of Americ (MBCA) and Moody’s Analytics. E.F.R. has received grants supported by NIAID U19AI12891303. N.G.R. has research grants from NIH, Pfizer, Merck, Sanofi, Quidel, and Lilly, and serves on safety committees for ICON and EMMES and the advisory boards of Moderna and Sanofi. Her institution has also received funding from NIH to conduct clinical trials of COVID-19 vaccines. J.S. received a grant from NIAID U19 for study implementation. A.C.S. has financial support from NIH U19 AI089992, NIH K24 AG042489. V.S. filed Patents at the Icahn School of Medicine at Mount Sinai relating to SARS-CoV-2 serological assays (the “Serology Assays” and NDV-based SARS-CoV-2 vaccines, which list V.S. as co-inventor. H.B. has received funding from NIH (Dengue Human Immunology Project Consortium - Mount Sinai IMPACC COVID-19 Cores), U19 AI118610 S1, NIH, CEIRR,75N93021C00014. SEB All funding sources are from NIH U19 AI090023-1S1, paid honoraria for serving on SAB for NIH NIAID P01AI174856-01, travel support from the University of Manitoba, and received TAK-242 from TAKEDA for pre-clinical testing. H.S. has received funding from 3 U19 AI 118608-05S3 through institution and travel support from NIAID. L.G. has received funding from Sean N. Parker Center for Allergy & Asthma Research, grants from Pfizer, and consulting fees from UnitedHealth Group. H.M. has received funding from NIH grant 2U19AI057229. R.D. has received grant support from UCSF COVID-19 Immunophenotyping Clinical Study and Core Laboratories (Grant number U19AI077439). V.S.M. has grants paid consulting as Vice Chair for EveryLife Foundation, Advisory board for Gemini labs, and stocks at My Own Med, Inc., d/b/a Respond Health. The remaining authors declare no competing interests.
Figures
References
-
- COVID-19 rapid guideline: managing the long-term effects of COVID-19. https://www.nice.org.uk/guidance/ng188. (2022). - PubMed
-
- National Institute for Health and Care Excellence: Clinical Guidelines. COVID-19 rapid guideline: managing the long-term effects of COVID-19. London: National Institute for Health and Care Excellence (NICE) Copyright © NICE 2020. (2020). - PubMed
Publication types
MeSH terms
Grants and funding
- U19 AI090023/AI/NIAID NIH HHS/United States
- U54 AI142766/AI/NIAID NIH HHS/United States
- U19 AI057229/AI/NIAID NIH HHS/United States
- R01 AI135201/AI/NIAID NIH HHS/United States
- S10 OD026880/OD/NIH HHS/United States
- U01 HL163124/HL/NHLBI NIH HHS/United States
- U19 AI062629/AI/NIAID NIH HHS/United States
- U19 AI077439/AI/NIAID NIH HHS/United States
- U19 AI118610/AI/NIAID NIH HHS/United States
- U19 AI128910/AI/NIAID NIH HHS/United States
- U19 AI167891/AI/NIAID NIH HHS/United States
- U19 AI167903/AI/NIAID NIH HHS/United States
- U19 AI125357/AI/NIAID NIH HHS/United States
- R01 AI145835/AI/NIAID NIH HHS/United States
- U19 AI128913/AI/NIAID NIH HHS/United States
- R01 AI132774/AI/NIAID NIH HHS/United States
- U19 AI118608/AI/NIAID NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- P01 AI153559/AI/NIAID NIH HHS/United States
- S10 OD030463/OD/NIH HHS/United States
- R01 AI135803/AI/NIAID NIH HHS/United States
- U19 AI089992/AI/NIAID NIH HHS/United States
- S10 OD030363/OD/NIH HHS/United States
- R01 AI104870/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
