

Accessibility of osteochondral lesion at the capitellum during elbow arthroscopy: an anatomical study
- PMID: 38172435
- PMCID: PMC10896769
- DOI: 10.1007/s00402-023-05172-7
Accessibility of osteochondral lesion at the capitellum during elbow arthroscopy: an anatomical study
Abstract
Introduction: Osteochondrosis dissecans (OCD) at the capitellum is a common pathology in young patients. Although arthroscopic interventions are commonly used, there is a lack of information about the accessibility of the defects during elbow arthroscopy by using standard portals.
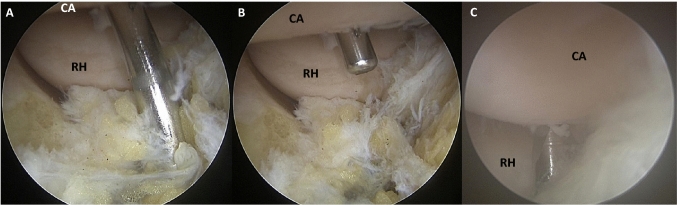
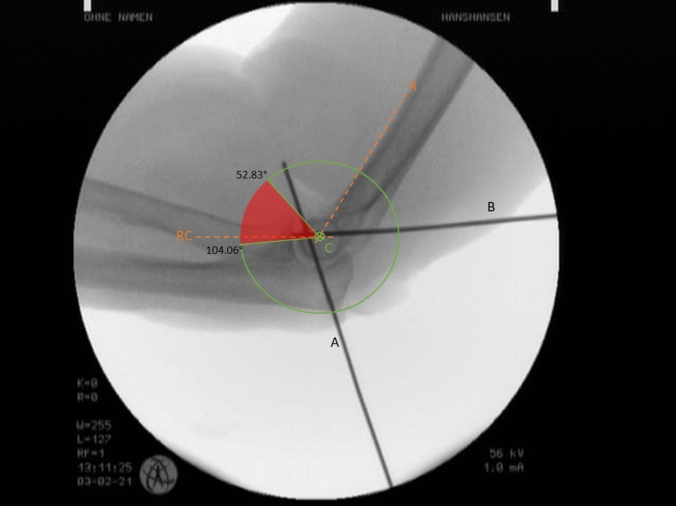
Materials and methods: An elbow arthroscopy using the standard portals was performed in seven fresh frozen specimens. At the capitellum, the most posterior and anterior cartilage surface reachable was marked with K-wires. Using a newly described measuring method, we constructed a circular sector around the rotational center of the capitellum. The intersection of K-wire "A" and "B" with the circular sector was marked, and the angles between the K-wires and the Rogers line, alpha angle for K-Wire "A" and beta angle for K-wire "B", and the corridor not accessible during arthroscopy was digitally measured.
Results: On average, we found an alpha angle of 53° and a beta angle of 104°. Leaving a sector of 51° which was not accessible via the standard portals during elbow arthroscopy.
Conclusion: Non-accessible capitellar lesions during elbow arthroscopy should be considered preoperatively, and the informed consent discussion should always include the possibility of open procedures or the use of flexible instruments.
Keywords: Arthroscopy; Elbow; Nanodrilling; Osteochondrosis dissecans.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Müller LP, Hollinger B, Burkhart KJ. Expertise Ellenbogen. Stuttgart: Georg Thieme Verlag; 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
