

Resting-state EEG measures cognitive impairment in Parkinson's disease
- PMID: 38172519
- PMCID: PMC10764756
- DOI: 10.1038/s41531-023-00602-0
Resting-state EEG measures cognitive impairment in Parkinson's disease
Abstract
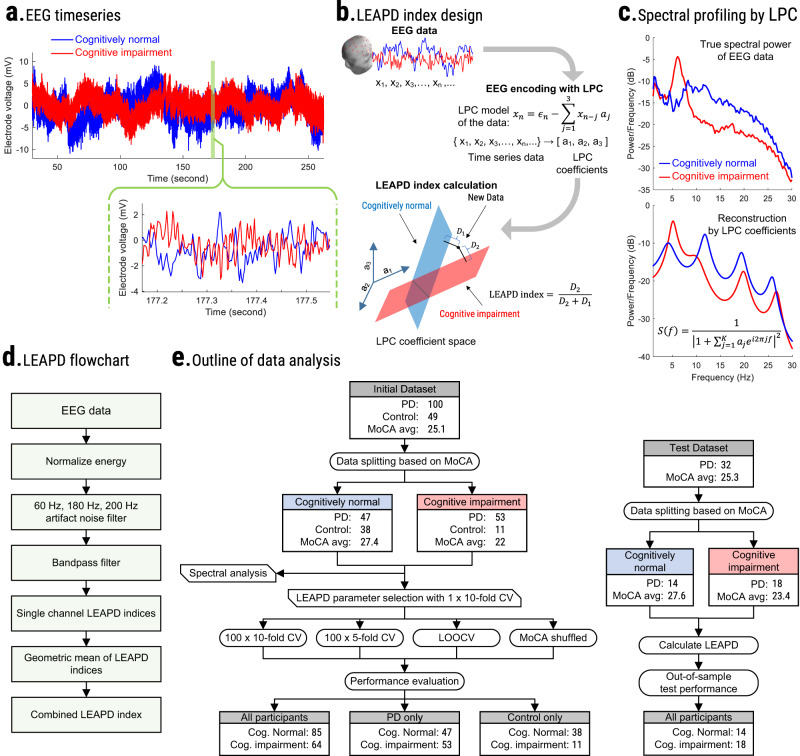
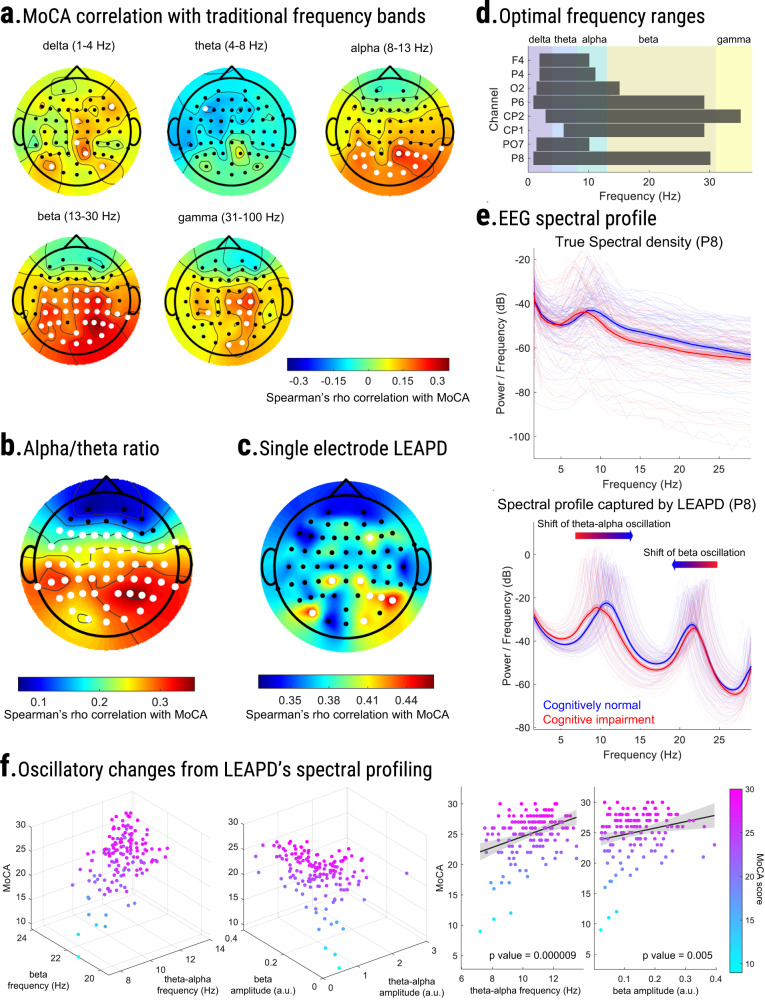
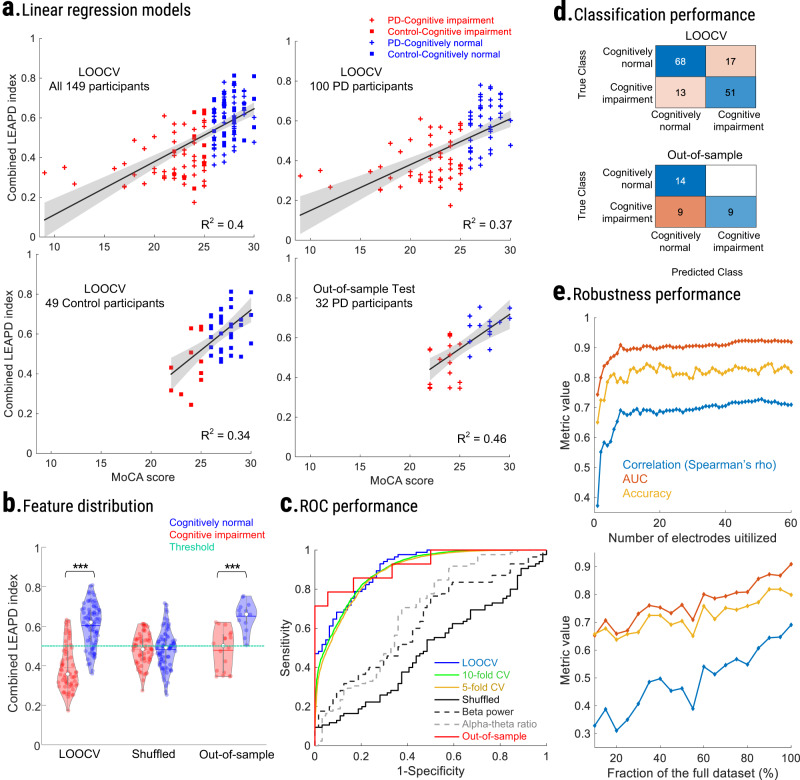
Cognitive dysfunction is common in Parkinson's disease (PD). We developed and evaluated an EEG-based biomarker to index cognitive functions in PD from a few minutes of resting-state EEG. We hypothesized that synchronous changes in EEG across the power spectrum can measure cognition. We optimized a data-driven algorithm to efficiently capture these changes and index cognitive function in 100 PD and 49 control participants. We compared our EEG-based cognitive index with the Montreal cognitive assessment (MoCA) and cognitive tests across different domains from National Institutes of Health (NIH) Toolbox using cross-validations, regression models, and randomization tests. Finally, we externally validated our approach on 32 PD participants. We observed cognition-related changes in EEG over multiple spectral rhythms. Utilizing only 8 best-performing electrodes, our proposed index strongly correlated with cognition (MoCA: rho = 0.68, p value < 0.001; NIH-Toolbox cognitive tests: rho ≥ 0.56, p value < 0.001) outperforming traditional spectral markers (rho = -0.30-0.37). The index showed a strong fit in regression models (R2 = 0.46) with MoCA, yielded 80% accuracy in detecting cognitive impairment, and was effective in both PD and control participants. Notably, our approach was equally effective (rho = 0.68, p value < 0.001; MoCA) in out-of-sample testing. In summary, we introduced a computationally efficient data-driven approach for cross-domain cognition indexing using fewer than 10 EEG electrodes, potentially compatible with dynamic therapies like closed-loop neurostimulation. These results will inform next-generation neurophysiological biomarkers for monitoring cognition in PD and other neurological diseases.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
Resting-state EEG measures cognitive impairment in Parkinson's disease.Res Sq [Preprint]. 2023 Mar 20:rs.3.rs-2666578. doi: 10.21203/rs.3.rs-2666578/v1. Res Sq. 2023. Update in: NPJ Parkinsons Dis. 2024 Jan 3;10(1):6. doi: 10.1038/s41531-023-00602-0. PMID: 36993450 Free PMC article. Updated. Preprint.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
