

Development and validation of a novel combinatorial nomogram model to predict in-hospital deaths in heart failure patients
- PMID: 38172656
- PMCID: PMC10765573
- DOI: 10.1186/s12872-023-03683-0
Development and validation of a novel combinatorial nomogram model to predict in-hospital deaths in heart failure patients
Abstract
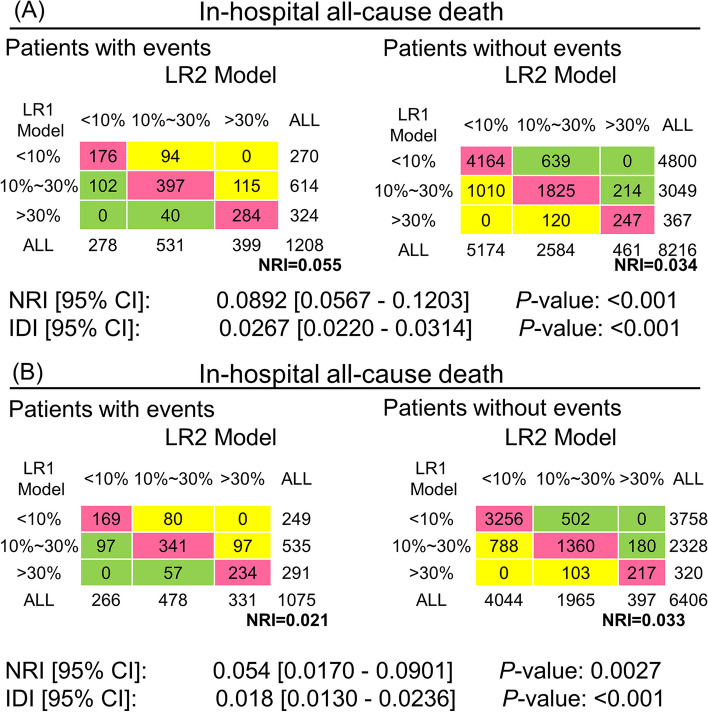
Background: The purpose of this study was to develop a Nomogram model to identify the risk of all-cause mortality during hospitalization in patients with heart failure (HF).
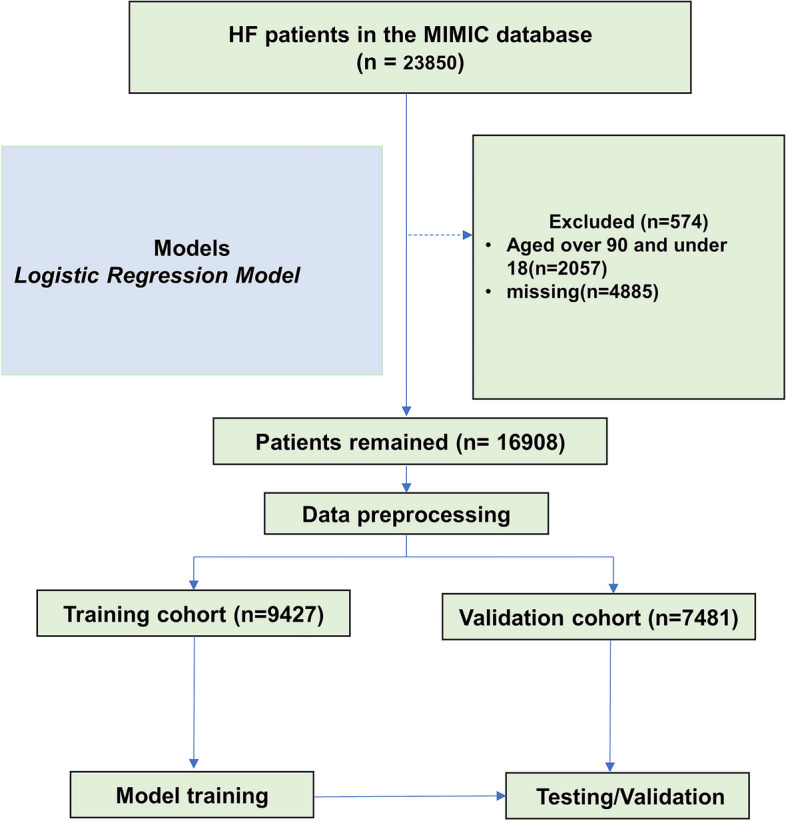
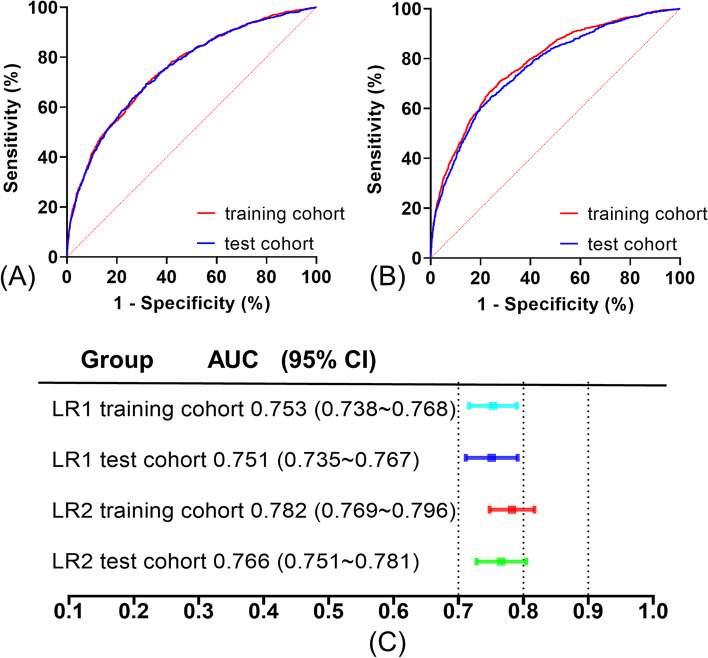
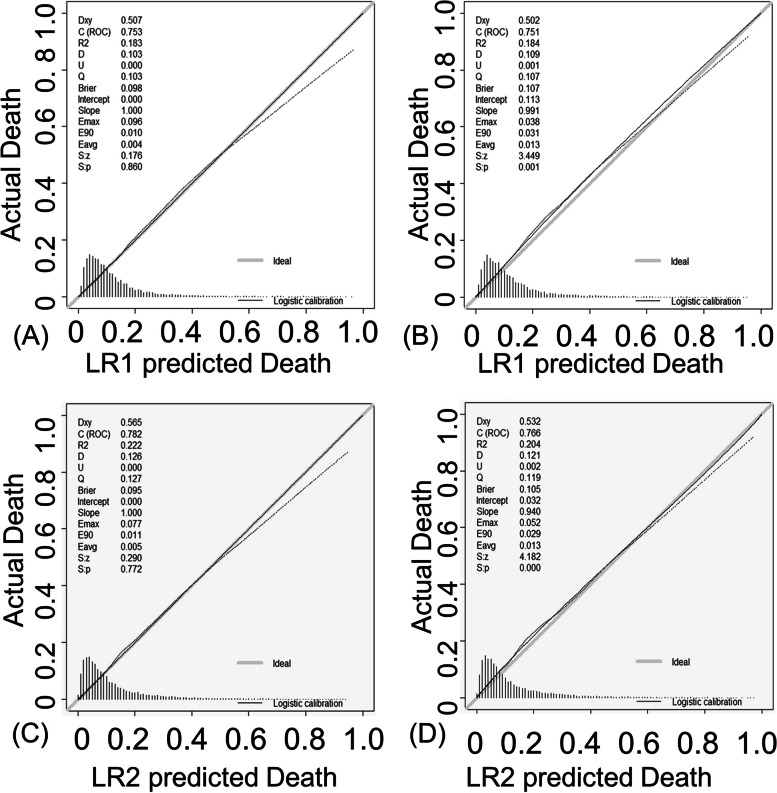
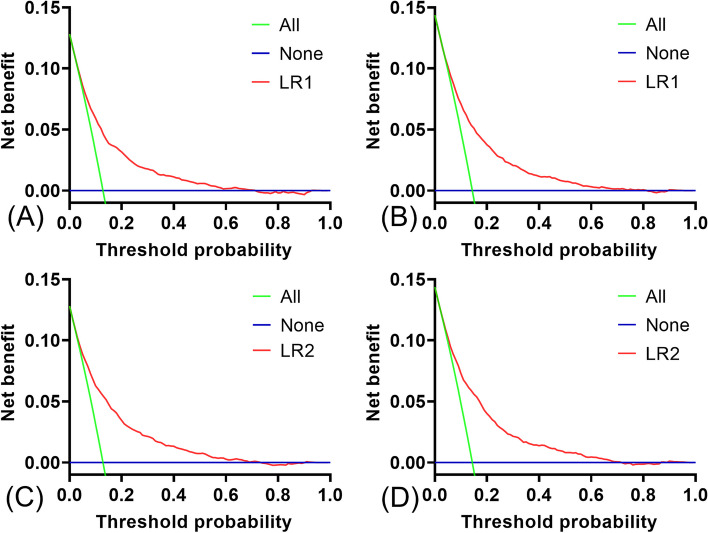
Methods: HF patients who had been registered in the Medical Information Mart for Intensive Care (MIMIC) III and IV databases were included. The primary outcome was the occurrence of all-cause mortality during hospitalization. Two Logistic Regression models (LR1 and LR2) were developed to predict in-hospital death for HF patients from the MIMIC-IV database. The MIMIC-III database were used for model validation. The area under the receiver operating characteristic curve (AUC) was used to compare the discrimination of each model. Calibration curve was used to assess the fit of each developed models. Decision curve analysis (DCA) was used to estimate the net benefit of the predictive model.
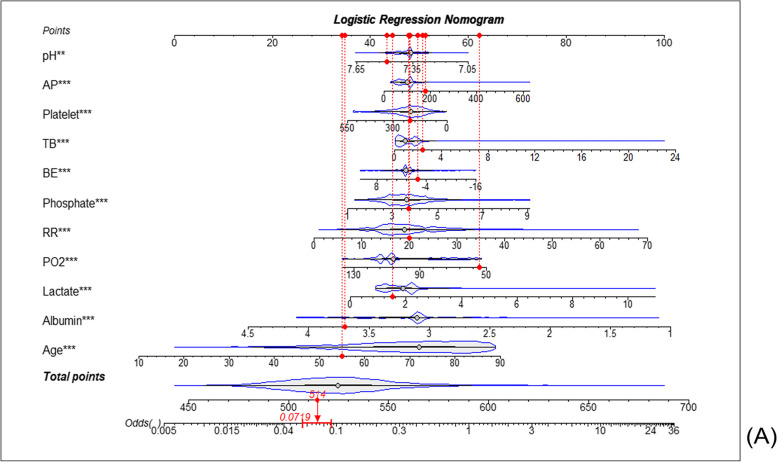
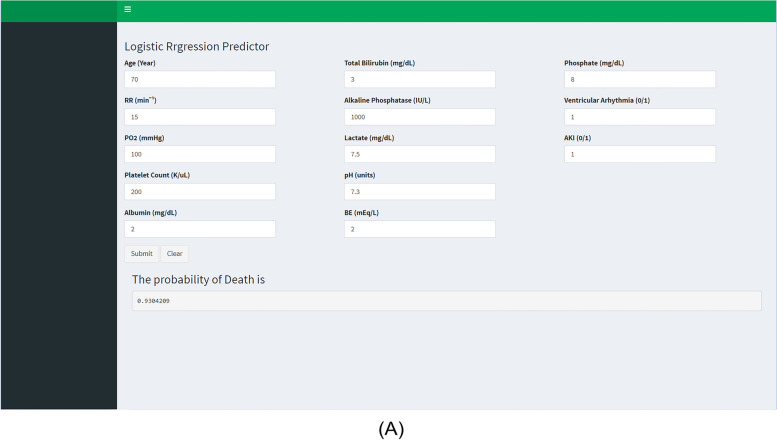
Results: A total of 16,908 HF patients were finally enrolled through screening, of whom 2,283 (13.5%) presented with in-hospital death. Totally, 48 variables were included and analyzed in the univariate and multifactorial regression analysis. The AUCs for the LR1 and LR2 models in the test cohort were 0.751 (95% CI: 0.735∼0.767) and 0.766 (95% CI: 0.751-0.781), respectively. Both LR models performed well in the calibration curve and DCA process. Nomogram and online risk assessment system were used as visualization of predictive models.
Conclusion: A new risk prediction tool and an online risk assessment system were developed to predict mortality in HF patients, which performed well and might be used to guide clinical practice.
Keywords: Heart failure; In-hospital death; Logistic regression; Medical information mart for intensive care; Nomogram.
© 2023. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose. The authors have no conflicts of interest to declare that are relevant to the content of this article. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript. The authors have no financial or proprietary interests in any material discussed in this article.
Figures
Similar articles
-
Machine learning prediction models and nomogram to predict the risk of in-hospital death for severe DKA: A clinical study based on MIMIC-IV, eICU databases, and a college hospital ICU.Int J Med Inform. 2023 Jun;174:105049. doi: 10.1016/j.ijmedinf.2023.105049. Epub 2023 Mar 27. Int J Med Inform. 2023. PMID: 37001474
-
Development of a novel tool: a nomogram for predicting in-hospital mortality of patients in intensive care unit after percutaneous coronary intervention.BMC Anesthesiol. 2023 Jan 6;23(1):5. doi: 10.1186/s12871-022-01923-y. BMC Anesthesiol. 2023. PMID: 36609220 Free PMC article. Clinical Trial.
-
A new nomogram to predict in-hospital mortality in patients with acute decompensated chronic heart failure and diabetes after 48 Hours of Intensive Care Unit.BMC Cardiovasc Disord. 2024 Apr 6;24(1):199. doi: 10.1186/s12872-024-03848-5. BMC Cardiovasc Disord. 2024. PMID: 38582861 Free PMC article.
-
A nomogram to predict the in-hospital mortality of patients with congestive heart failure and chronic kidney disease.ESC Heart Fail. 2022 Oct;9(5):3167-3176. doi: 10.1002/ehf2.14042. Epub 2022 Jun 28. ESC Heart Fail. 2022. PMID: 35765720 Free PMC article.
-
Development and validation a nomogram prediction model for early diagnosis of bloodstream infections in the intensive care unit.Front Cell Infect Microbiol. 2024 Mar 4;14:1348896. doi: 10.3389/fcimb.2024.1348896. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38500500 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
- CE20225051/Changzhou Sci&Tech Program
- 82270328/National Natural Science Foundation of China
- BK20221229/Natural Science Research of Jiangsu Higher Education Institutions of China
- 2022M720544/China Postdoctoral Science Funding Program
- 2022CZBJ054/Changzhou High-Level Medical Talents Training Project
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
