

Association between hemoglobin A1c and abdominal aortic calcification: results from the National Health and Nutrition Examination Survey 2013-2014
- PMID: 38172671
- PMCID: PMC10765683
- DOI: 10.1186/s12872-023-03700-2
Association between hemoglobin A1c and abdominal aortic calcification: results from the National Health and Nutrition Examination Survey 2013-2014
Abstract
Background: Hemoglobin A1c (HbA1c), a "gold standard" for the assessment of glycemic control, was associated with an increased risk of cardiovascular disease and coronary artery calcification. However, its effects on abdominal aortic calcification (AAC) are uncertain. The present study comprehensively investigated the association between HbA1c and AAC in the 2013-2014 National Health and Nutrition Examinations Surveys.
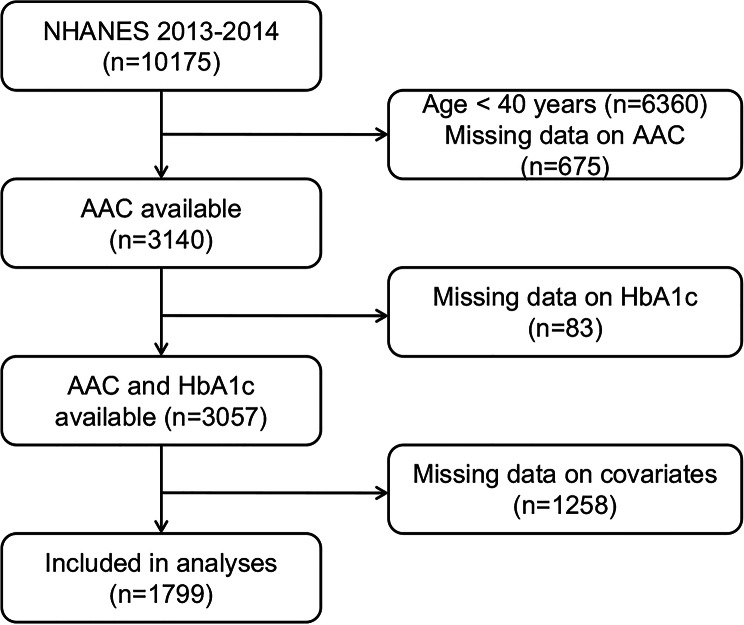
Methods: Among 1,799 participants ≥ 40 years, dual-energy X-ray absorptiometry-derived AAC was quantified using the Kauppila score (AAC-24). Severe AAC was defined as a total AAC-24 > 6. Weighted linear regression models and logistic regression models were used to determine the effects of HbA1c on AAC. The restricted cubic spline model was used for the dose-response analysis.
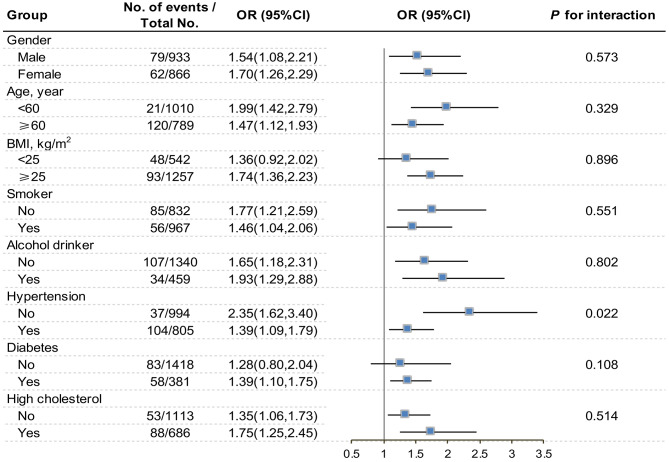
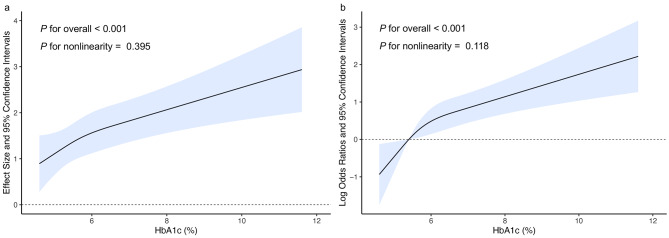
Results: The mean AAC-24 of participants was 1.3, and 6.7% of them suffered from severe AAC. Both AAC-24 and the prevalence of severe AAC increased with the higher tertile of HbA1c (P < 0.001). Elevated HbA1c levels would increase the AAC-24 (β = 0.73, 95% CI: 0.30-1.16) and the risk of severe AAC (OR = 1.63, 95% CI: 1.29-2.06), resulting in nearly linear dose-response relationships in all participants. However, this positive correlation were not statistically significant when participants with diabetes were excluded. Furthermore, subgroup analysis showed significant interactions effect between HbA1c and hypertension on severe AAC with the OR (95% CI) of 2.35 (1.62-3.40) for normotensives and 1.39 (1.09-1.79) for hypertensives (P for interaction = 0.022).
Conclusion: Controlling HbA1c could reduce AAC scores and the risk of severe AAC. Glycemic management might be a component of strategies for preventing AAC among all participants, especially normotensives.
Keywords: Abdominal aortic calcification; Cross-sectional study; Hemoglobin A1c; NHANES.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Association between the triglyceride-glucose index and abdominal aortic calcification in adults: A cross-sectional study.Nutr Metab Cardiovasc Dis. 2021 Jun 30;31(7):2068-2076. doi: 10.1016/j.numecd.2021.04.010. Epub 2021 Apr 19. Nutr Metab Cardiovasc Dis. 2021. PMID: 34053833
-
Association between Ward's triangle bone mineral density levels and abdominal aortic calcification: Data from the national health and nutrition examination survey 2013-2014.Clin Nutr ESPEN. 2024 Dec;64:344-357. doi: 10.1016/j.clnesp.2024.10.154. Epub 2024 Oct 24. Clin Nutr ESPEN. 2024. PMID: 39461592
-
Associations between bone mineral density and abdominal aortic calcification: Results of a nationwide survey.Nutr Metab Cardiovasc Dis. 2024 Jun;34(6):1488-1495. doi: 10.1016/j.numecd.2024.01.031. Epub 2024 Feb 7. Nutr Metab Cardiovasc Dis. 2024. PMID: 38494366
-
Prevalence of abdominal artery calcification in dialysis patients with end-stage renal disease: a systematic review and meta-analysis.Int Urol Nephrol. 2017 Nov;49(11):2061-2069. doi: 10.1007/s11255-017-1685-9. Epub 2017 Sep 21. Int Urol Nephrol. 2017. PMID: 28936714
-
Prognostic Value of Abdominal Aortic Calcification: A Systematic Review and Meta-Analysis of Observational Studies.J Am Heart Assoc. 2021 Jan 19;10(2):e017205. doi: 10.1161/JAHA.120.017205. Epub 2021 Jan 13. J Am Heart Assoc. 2021. PMID: 33439672 Free PMC article.
Cited by
-
Associations between oxidation balance score and abdominal aortic calcification, and the mediating role of glycohemoglobin: a nationally representative cross-sectional study from NHANES.Front Nutr. 2025 Jan 20;12:1469449. doi: 10.3389/fnut.2025.1469449. eCollection 2025. Front Nutr. 2025. PMID: 39906239 Free PMC article.
-
Poor Sleep Pattern Might Increase the Prevalence of Abdominal Aortic Calcification in US Adults: Data from the NHANES (2013-2014).Vasc Health Risk Manag. 2025 Jul 31;21:571-579. doi: 10.2147/VHRM.S532476. eCollection 2025. Vasc Health Risk Manag. 2025. PMID: 40771302 Free PMC article.
References
-
- Allam AHA, Thompson RC, Eskander MA, Mandour Ali MA, Sadek A, Rowan CJ, Sutherland ML, Sutherland JD, Frohlich B, Michalik DE, et al. Is coronary calcium scoring too late? Total body arterial calcium burden in patients without known CAD and normal MPI. J Nucl Cardiol. 2018;25(6):1990–8. doi: 10.1007/s12350-017-0925-9. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
