

Changes in tuberculosis risk after transplantation in the setting of decreased community tuberculosis incidence: a national population-based study, 2008-2020
- PMID: 38172897
- PMCID: PMC10765802
- DOI: 10.1186/s12941-023-00661-4
Changes in tuberculosis risk after transplantation in the setting of decreased community tuberculosis incidence: a national population-based study, 2008-2020
Abstract
Background: Transplant recipients are immunocompromised and vulnerable to developing tuberculosis. However, active tuberculosis incidence is rapidly declining in South Korea, but the trend of tuberculosis infection among transplant recipients has not been elucidated. This study aimed to evaluate the risk of active tuberculosis after transplantation, including risk factors for tuberculosis and standardized incidence ratios, compared with that in the general population.
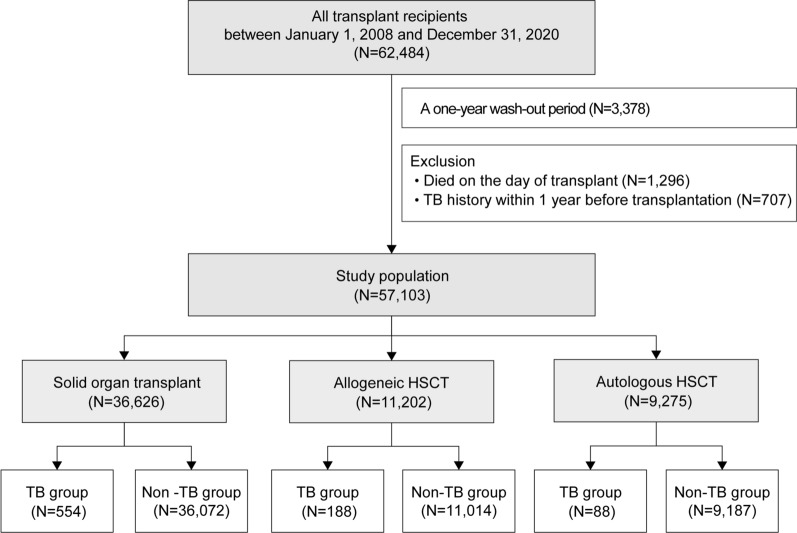
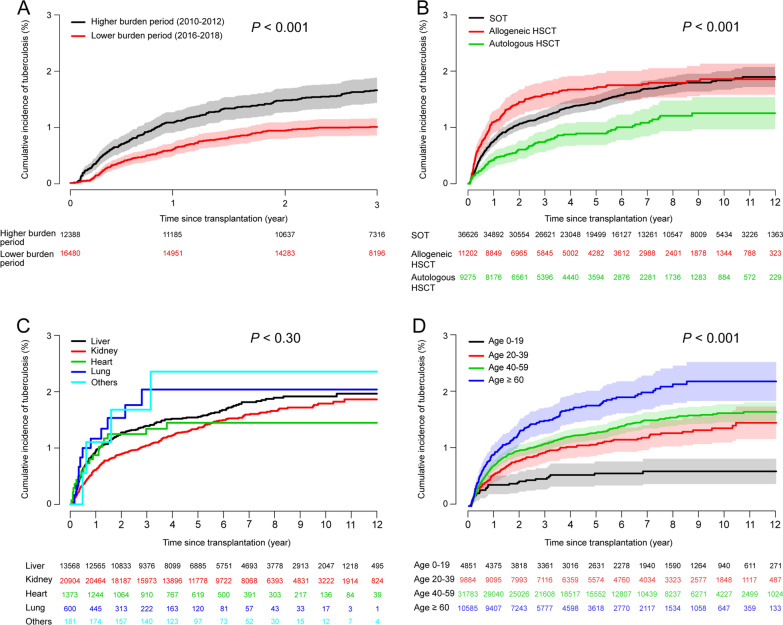
Methods: This retrospective study was conducted based on the South Korean health insurance review and assessment database among those who underwent transplantation (62,484 recipients) between 2008 and 2020. Tuberculosis incidence was compared in recipients treated during higher- (2010-2012) and lower-disease burden (2016-2018) periods. Standardized incidence ratios were analyzed using the Korean Tuberculosis Surveillance System. The primary outcome was the number of new tuberculosis cases after transplantation.
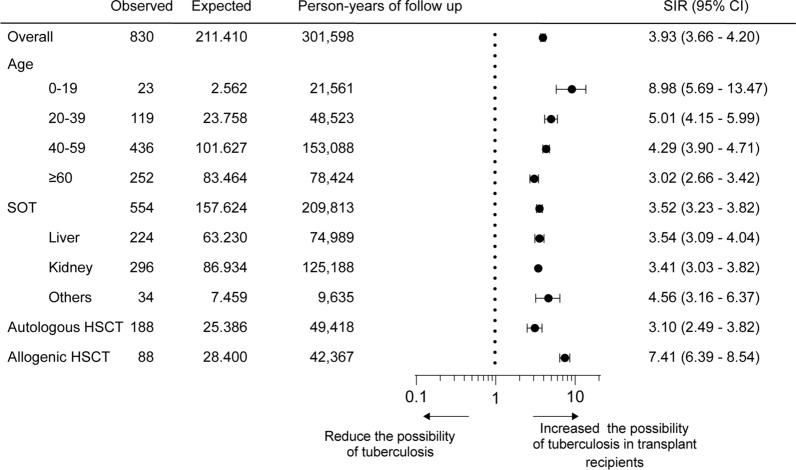
Results: Of 57,103 recipients analyzed, the overall cumulative incidence rate 1 year after transplantation was 0.8% (95% confidence interval [CI]: 0.7-0.8), significantly higher in the higher-burden period than in the lower-burden period (1.7% vs. 1.0% 3 years after transplantation, P < 0.001). Individuals who underwent allogeneic hematopoietic stem cell transplantation had the highest tuberculosis incidence, followed by those who underwent solid organ transplantation and autologous hematopoietic stem cell transplantation (P < 0.001). The overall standardized incidence ratio was 3.9 (95% CI 3.7-4.2) and was the highest in children aged 0-19 years, at 9.0 (95% CI 5.7-13.5). Male sex, older age, tuberculosis history, liver transplantation, and allogeneic hematopoietic stem cell transplantation were risk factors for tuberculosis.
Conclusions: Transplant recipients are vulnerable to developing tuberculosis, possibly influenced by their immunocompromised status, solid organ transplant type, age, and community prevalence of tuberculosis. Tuberculosis prevalence by country, transplant type, and age should be considered to establish an appropriate tuberculosis prevention strategy for high-risk groups.
Keywords: Community tuberculosis burden; Hematopoietic stem cell transplantation; Solid organ transplantation; Standardized incidence ratio; Tuberculosis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization . Global tuberculosis report 2022. Geneva: World Health Organization; 2022.
-
- Aguado JM, Herrero JA, Gavaldá J, Torre-Cisneros J, Blanes M, Rufí G, et al. Clinical presentation and outcome of tuberculosis in kidney, liver, and heart transplant recipients in Spain. Spanish Transplantation Infection Study Group, GESITRA. Transplantation. 1997;63(9):1278–1286. doi: 10.1097/00007890-199705150-00015. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
