

Single-drug versus combination antimicrobial therapy in critically ill patients with hospital-acquired pneumonia and ventilator-associated pneumonia due to Gram-negative pathogens: a multicenter retrospective cohort study
- PMID: 38172969
- PMCID: PMC10765858
- DOI: 10.1186/s13054-023-04792-0
Single-drug versus combination antimicrobial therapy in critically ill patients with hospital-acquired pneumonia and ventilator-associated pneumonia due to Gram-negative pathogens: a multicenter retrospective cohort study
Abstract
Key messages: In this study including 391 critically ill patients with nosocomial pneumonia due to Gram-negative pathogens, combination therapy was not associated with a reduced hazard of death at Day 28 or a greater likelihood of clinical cure at Day 14. No over-risk of AKI was observed in patients receiving combination therapy.
Background: The benefits and harms of combination antimicrobial therapy remain controversial in critically ill patients with hospital-acquired pneumonia (HAP), ventilated HAP (vHAP) or ventilator-associated pneumonia (VAP) involving Gram-negative bacteria.
Methods: We included all patients in the prospective multicenter OutcomeRea database with a first HAP, vHAP or VAP due to a single Gram-negative bacterium and treated with initial adequate single-drug or combination therapy. The primary endpoint was Day-28 all-cause mortality. Secondary endpoints were clinical cure rate at Day 14 and a composite outcome of death or treatment-emergent acute kidney injury (AKI) at Day 7. The average effects of combination therapy on the study endpoints were investigated through inverse probability of treatment-weighted regression and multivariable regression models. Subgroups analyses were performed according to the resistance phenotype of the causative pathogens (multidrug-resistant or not), the pivotal (carbapenems or others) and companion (aminoglycosides/polymyxins or others) drug classes, the duration of combination therapy (< 3 or ≥ 3 days), the SOFA score value at pneumonia onset (< 7 or ≥ 7 points), and in patients with pneumonia due to non-fermenting Gram-negative bacteria, pneumonia-related bloodstream infection, or septic shock.
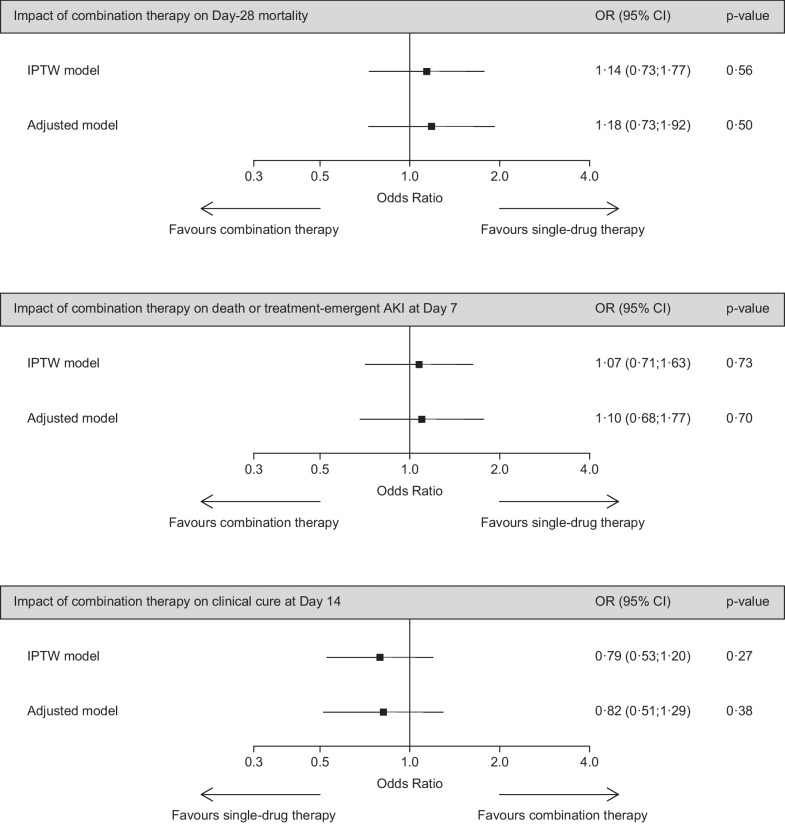
Results: Among the 391 included patients, 151 (38.6%) received single-drug therapy and 240 (61.4%) received combination therapy. VAP (overall, 67.3%), vHAP (16.4%) and HAP (16.4%) were equally distributed in the two groups. All-cause mortality rates at Day 28 (overall, 31.2%), clinical cure rate at Day 14 (43.7%) and the rate of death or AKI at Day 7 (41.2%) did not significantly differ between the groups. In inverse probability of treatment-weighted analyses, combination therapy was not independently associated with the likelihood of all-cause death at Day 28 (adjusted odd ratio [aOR], 1.14; 95% confidence interval [CI] 0.73-1.77; P = 0.56), clinical cure at Day 14 (aOR, 0.79; 95% CI 0.53-1.20; P = 0.27) or death or AKI at Day 7 (aOR, 1.07; 95% CI 0.71-1.63; P = 0.73). Multivariable regression models and subgroup analyses provided similar results.
Conclusions: Initial combination therapy exerts no independent impact on Day-28 mortality, clinical cure rate at Day 14, and the hazard of death or AKI at Day 7 in critically ill patients with mono-bacterial HAP, vHAP or VAP due to Gram-negative bacteria.
Keywords: Antimicrobial stewardship; Antimicrobial therapy; De-escalation; Enterobacterales; Hospital-acquired pneumonia; Intensive care unit; Outcome; Pseudomonas aeruginosa; Ventilator-associated pneumonia.
© 2024. The Author(s).
Conflict of interest statement
F. B. declares having received lecture and consulting fees from MSD, lecture fees for BioMérieux and conference invitation from Pfizer, not related to the submitted work. J.-F. T. declares having received consulting fees from Gilead, MSD, Pfizer, BioMérieux and Roche diagnostic, and lecture fees from MSD, Pfizer, Shionogi, BioMérieux, Qiagen, Mundipharma and Gilead, not related to the submitted work. J.-R. Z. declares having received consulting fees and conference invitation from MSD, consulting fees, lecture fees and conference invitations from Pfizer, lecture Fees from Advanz-Pharma and Shionogui, and conference invitations from Biomérieux and Gilead, not related to the submitted work. E. A. is Associate Editor of
Figures

References
-
- Torres A, Niederman MS, Chastre J, Ewig S, Fernandez-Vandellos P, Hanberger H, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT) Eur Respir J. 2017;50(3):1700582. doi: 10.1183/13993003.00582-2017. - DOI - PubMed
-
- Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61–111. doi: 10.1093/cid/ciw353. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
