

Indications for alternative endovascular techniques in carotid-cavernous fistulas: A 20-year single-center experience
- PMID: 38173239
- PMCID: PMC11569750
- DOI: 10.1177/15910199231217549
Indications for alternative endovascular techniques in carotid-cavernous fistulas: A 20-year single-center experience
Abstract
Background: While coiling is considered the standard treatment for carotid-cavernous fistulas (CCFs), studies demonstrating excellent results using new materials, especially flow diverter (FD) stents and liquid embolisates, are becoming more frequent. The indications and effectiveness of these alternative endovascular techniques remain unclear.
Methods: A total of 22 direct and 20 indirect CCFs were included in the study. These were further subdivided based on the embolic material used: coils versus FD stents for direct and coils versus liquid embolisates for indirect CCFs. The subgroups were subjected to statistical analysis.
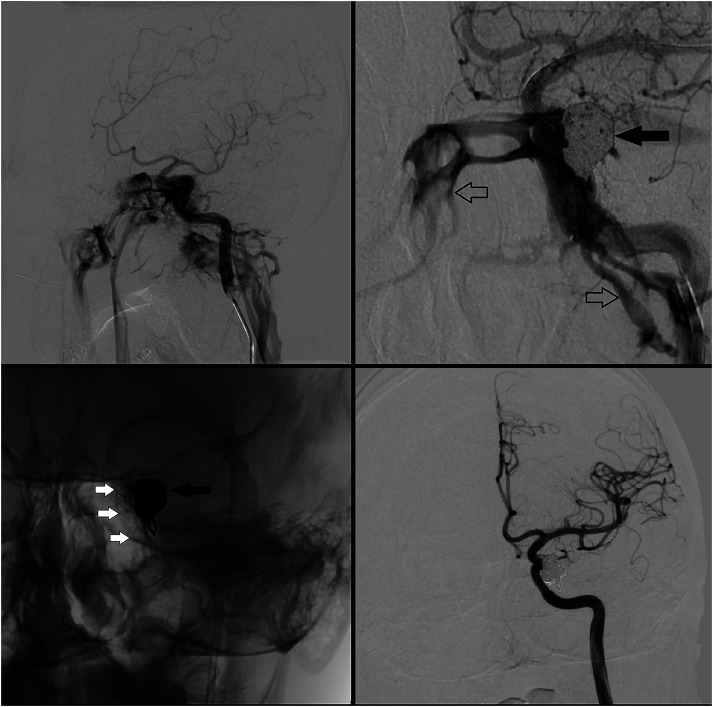
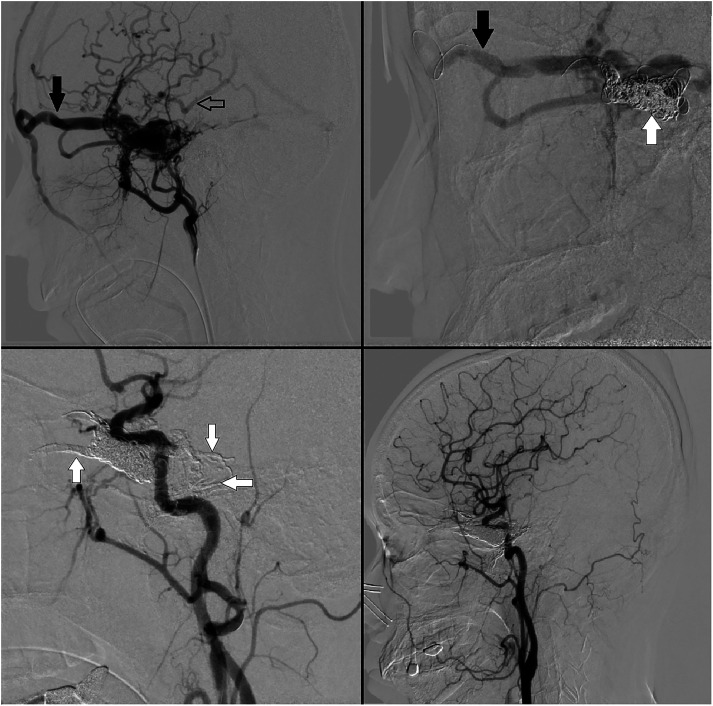
Results: An angiographic cure was achieved in 88% of all CCFs, 93% of patients' experienced clinical improvement or remained stable. Direct CCFs were treated with coiling (41%) or with both coils and FD stents (55%). One (4%) patient with a direct CCF was treated with FD stent alone. Statistical analysis comparing these subgroups revealed a significantly higher complete occlusion rate immediately after treatment in the coiling subgroup (67% vs. 23%, p = 0.0409). The occlusion rates at the last follow-up were similar (89% vs. 85%). Indirect CCFs were treated with coiling (35%) or liquid embolisates (65%). All three periprocedural ischemic complications were recorded within the liquid subgroup, resulting in a significantly higher clinical deterioration rate (p = 0.0333).
Conclusion: FD stents in direct and liquid embolisates in indirect fistulas did not demonstrate better angiographic or clinical outcomes compared to convetional coiling. Liquid agents carried a higher risk of ischemic complications. Alternative embolization materials should be reserved for CCFs that cannot be treated with simple coiling.
Keywords: Carotid-cavernous fistula; embolization; flow-diverter devices; liquid embolisates.
Conflict of interest statement
Declaration of conflicting interestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Flow diversion for indirect carotid-cavernous fistula: Still an off-label indication?Surg Neurol Int. 2023 Feb 24;14:65. doi: 10.25259/SNI_1113_2022. eCollection 2023. Surg Neurol Int. 2023. PMID: 36895234 Free PMC article.
-
Long-term outcome of endovascular treatment for indirect carotid-cavernous fistulas.Neurosurg Focus. 2024 Mar;56(3):E5. doi: 10.3171/2023.12.FOCUS23795. Neurosurg Focus. 2024. PMID: 38427986
-
Efficiency of endovascular management with a combination of Onyx and coils for direct and indirect carotid cavernous fistula treatment: Experience of a single center.Clin Neurol Neurosurg. 2023 May;228:107700. doi: 10.1016/j.clineuro.2023.107700. Epub 2023 Mar 27. Clin Neurol Neurosurg. 2023. PMID: 36996671
-
Endovascular techniques for treatment of carotid-cavernous fistula.J Neuroophthalmol. 2009 Mar;29(1):62-71. doi: 10.1097/WNO.0b013e3181989fc0. J Neuroophthalmol. 2009. PMID: 19458580 Review.
-
Carotid cavernous fistulas treated by endovascular covered stent grafts with follow-up results.Br J Neurosurg. 2010 Aug;24(4):435-40. doi: 10.3109/02688697.2010.487127. Br J Neurosurg. 2010. PMID: 20515263 Review.
References
-
- Barrow DL, Spector RH, Landman JA, et al. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg 1985; 62: 248–256. - PubMed
-
- d’Angelo VA, Monte V, Scialfa G, et al. Intracerebral venous hemorrhage in “high-risk” carotid-cavernous fistula. Surg Neurol 1988; 30: 387–390. - PubMed
-
- Ellis JA, Goldstein H, Connolly ES, Jr, et al. Carotid-cavernous fistulas. Neurosurg Focus 2012; 32: E9. - PubMed
-
- Lang M, Habboub G, Mullin JP, et al. A brief history of carotid-cavernous fistula. J Neurosurg 2016; 126: 1995–2001. - PubMed
-
- Serbinenko FA. Balloon catheterization and occlusion of major cerebral vessels. J Neurosurg 1974; 41: 125–145. - PubMed
LinkOut - more resources
Full Text Sources
