

Anatomical Distribution Patterns of Peripheral Arterial Disease in the Upper Extremities According to Patient Characteristics: A Retrospective Cohort Study
- PMID: 38173811
- PMCID: PMC10762427
- DOI: 10.2147/VHRM.S440408
Anatomical Distribution Patterns of Peripheral Arterial Disease in the Upper Extremities According to Patient Characteristics: A Retrospective Cohort Study
Abstract
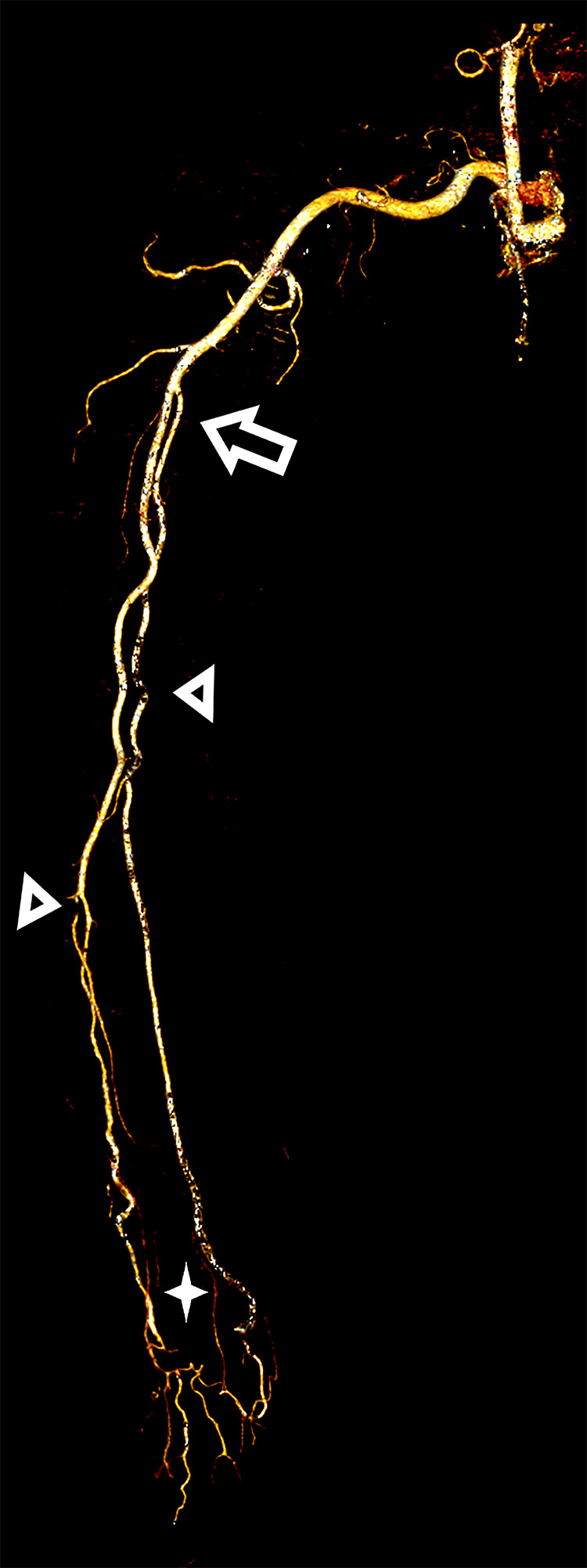
Purpose: Peripheral arterial disease (PAD) greatly affects the patients' quality of life. We aimed to investigate the affected anatomical sites and distribution patterns in upper extremity PAD using computed tomography angiography (CTA). Furthermore, we sought to identify the correlations between patient characteristics and the identified patterns.
Patients and methods: This was a retrospective chart review of upper limb CTA findings from patients with symptomatic PAD aged >18 years. Significant variables from univariate logistic regression analysis were further tested using multivariate logistic regression analysis. Statistical significance was set at p < 0.05, with confidence intervals of 95%.
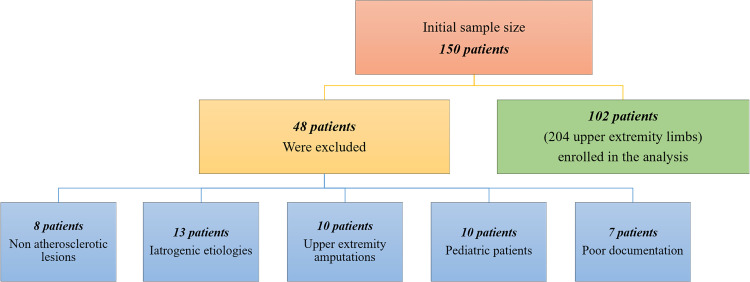
Results: The mean age of the 102 included patients with upper extremity PAD was 55.45 years. Laterality analysis revealed that the upper left limb segments were more affected than the upper right limb segments (42 vs 63; left-to-right ratio, 3:2). The forearm was the segment most affected by stenotic PAD (62 segments, 3.37%). The arm was the segment most affected by occlusive PAD (14 segments, 0.76%). Diabetes mellitus (DM) and hypertension (HTN) were significant predictors of PAD (p = 0.046). In patients with DM, the occlusive form of PAD was dominant in the arm (18.18%); however, the stenotic form prevailed in the forearm (72.72%). In patients with HTN, the occlusive form of PAD was predominant in the arm (45.45%); however, the stenotic form tended to occur in the arm and forearm (90.90%).
Conclusion: The distribution patterns of upper extremity PAD are linked to its underlying pathophysiology. HTN and DM are the most frequent comorbidities in patients with upper extremity PAD. Angiographically, PAD in these patients is likely to present as stenosis rather than as occlusion. This is vital for interventionists who deviate from radial arterial access in patients with PAD. Therefore, targeted screening standards are required, and further studies on PAD are warranted.
Keywords: angiography; computed tomography; diabetes mellitus; hypertension; stenosis.
© 2023 Al-Sharydah et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Anatomical Distribution Patterns of Peripheral Arterial Disease According to Patient Characteristics: A Unicentral Cohort Study.Vasc Health Risk Manag. 2023 Jul 17;19:447-457. doi: 10.2147/VHRM.S416967. eCollection 2023. Vasc Health Risk Manag. 2023. PMID: 37485230 Free PMC article.
-
Stenting for peripheral artery disease of the lower extremities: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(18):1-88. Epub 2010 Sep 1. Ont Health Technol Assess Ser. 2010. PMID: 23074395 Free PMC article.
-
Accuracy of Noncontrast Quiescent-Interval Single-Shot Lower Extremity MR Angiography Versus CT Angiography for Diagnosis of Peripheral Artery Disease: Comparison With Digital Subtraction Angiography.JACC Cardiovasc Imaging. 2017 Oct;10(10 Pt A):1116-1124. doi: 10.1016/j.jcmg.2016.09.030. Epub 2017 Jan 18. JACC Cardiovasc Imaging. 2017. PMID: 28109932
-
A Review of Distribution of Atherosclerosis in the Lower Limb Arteries of Patients With Diabetes Mellitus and Peripheral Vascular Disease.Vasc Endovascular Surg. 2018 Oct;52(7):535-542. doi: 10.1177/1538574418791622. Epub 2018 Aug 1. Vasc Endovascular Surg. 2018. PMID: 30068238 Review.
-
Pathophysiology of peripheral arterial disease in diabetes mellitus.J Diabetes. 2017 Feb;9(2):133-140. doi: 10.1111/1753-0407.12474. Epub 2016 Oct 13. J Diabetes. 2017. PMID: 27556728 Review.
Cited by
-
"Y" Configuration of the Arterial Pedicle or the Use of a Saphenous Vein Graft for Microsurgical Reconstruction in the Old and Diseased-A Retrospective Study.J Clin Med. 2024 Dec 30;14(1):157. doi: 10.3390/jcm14010157. J Clin Med. 2024. PMID: 39797239 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
