

Brain herniation and subsequent complications following partial resection of high-grade glioma: A case report
- PMID: 38173889
- PMCID: PMC10762324
- DOI: 10.1002/ccr3.8407
Brain herniation and subsequent complications following partial resection of high-grade glioma: A case report
Abstract
Key clinical message: This case highlights the need for tailored strategies to address issues like brain herniation, subdural hygroma, and cerebrospinal fluid leak, which, if not managed promptly, can lead to long-term neurological deficits. Additionally, the role of specialized facilities in delivering highly specialized care for managing such intricate cases cannot be understated.
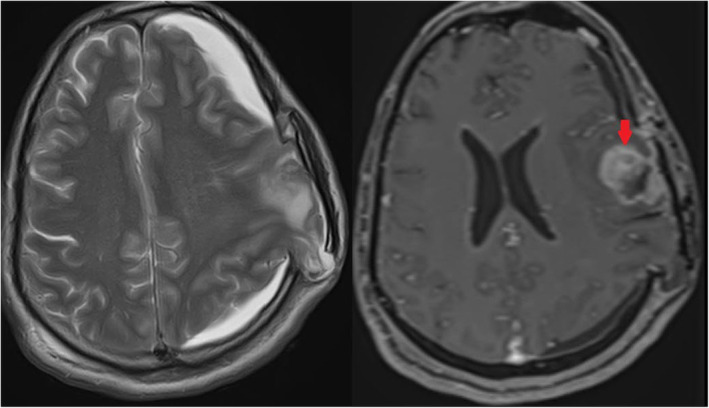
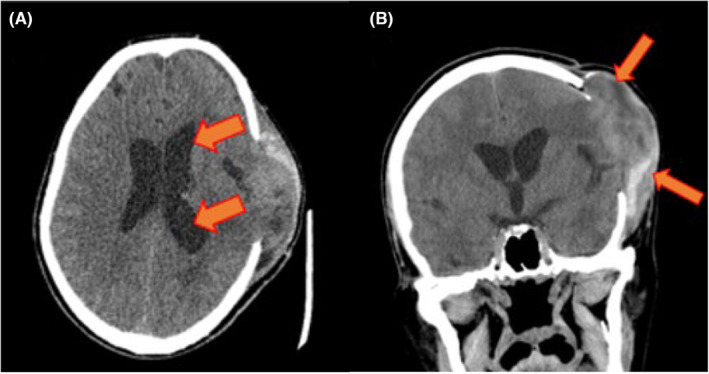
Abstract: Decompressive craniectomy-induced subdural hygroma (SDH) frequently coexists with external cerebral herniation, resulting in neurological impairments. The incidence of brain herniation through a craniectomy defect postoperatively is 25%. Brain herniation (BH), SDH, and cerebrospinal fluid leak require urgent neurosurgical management as they can lead to irreversible long-term neurological deficits. We report a case of a 42-year-old male who presented with headache and grand mal seizures. He was diagnosed with herniation of brain parenchyma through the surgical defect with a displacement of the bone flap by a heterogeneously enhancing lesion in the left parietal lobe along with SDH in the left frontoparietal region post partial resection of high-grade glioma. In this report, we discuss the pathogenesis and management strategies of brain herniation, wound infection, cerebrospinal fluid (CSF) leak, ipsilateral SDH, floating bone flap, and communicating hydrocephalus in an adult patient following partial resection of high-grade glioma. This particular case emphasizes the value of an individualized patient-centered surgical approach to minimize the risk of postoperative complications.
Keywords: elevated intracranial pressure; glial cell neoplasms; glial cell tumor; intracranial hypertension; skull excision; subdural cerebrospinal fluid effusion; subdural cerebrospinal fluid leakage.
© 2024 The Authors. Clinical Case Reports published by John Wiley & Sons Ltd.
Figures

References
-
- Sukesh P, Meena, Chandrika P. Behavioural and cognitive symptom manifestation in a case of subdural hygroma. Indian J Psychiatry. 2022;64(Suppl 3):S689‐S690. doi:10.4103/0019-5545.342036 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
