

Luxembourg Parkinson's study -comprehensive baseline analysis of Parkinson's disease and atypical parkinsonism
- PMID: 38174101
- PMCID: PMC10763250
- DOI: 10.3389/fneur.2023.1330321
Luxembourg Parkinson's study -comprehensive baseline analysis of Parkinson's disease and atypical parkinsonism
Abstract
Background: Deep phenotyping of Parkinson's disease (PD) is essential to investigate this fastest-growing neurodegenerative disorder. Since 2015, over 800 individuals with PD and atypical parkinsonism along with more than 800 control subjects have been recruited in the frame of the observational, monocentric, nation-wide, longitudinal-prospective Luxembourg Parkinson's study.
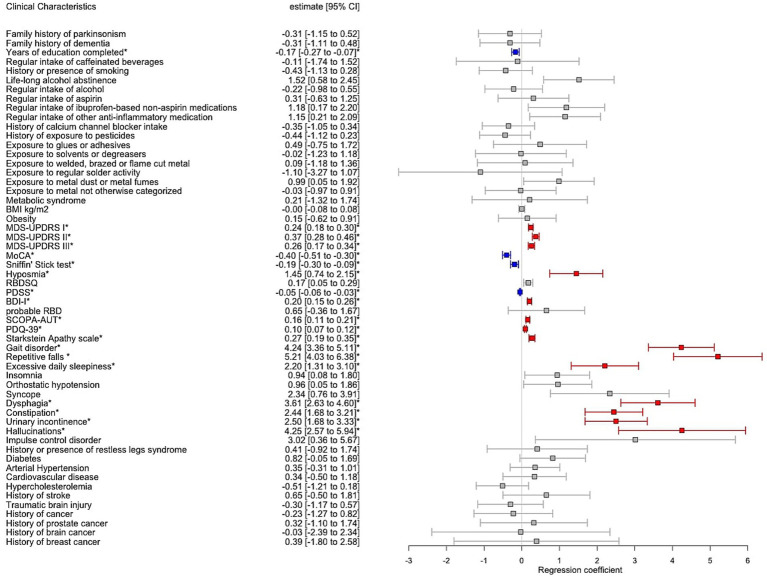
Objective: To profile the baseline dataset and to explore risk factors, comorbidities and clinical profiles associated with PD, atypical parkinsonism and controls.
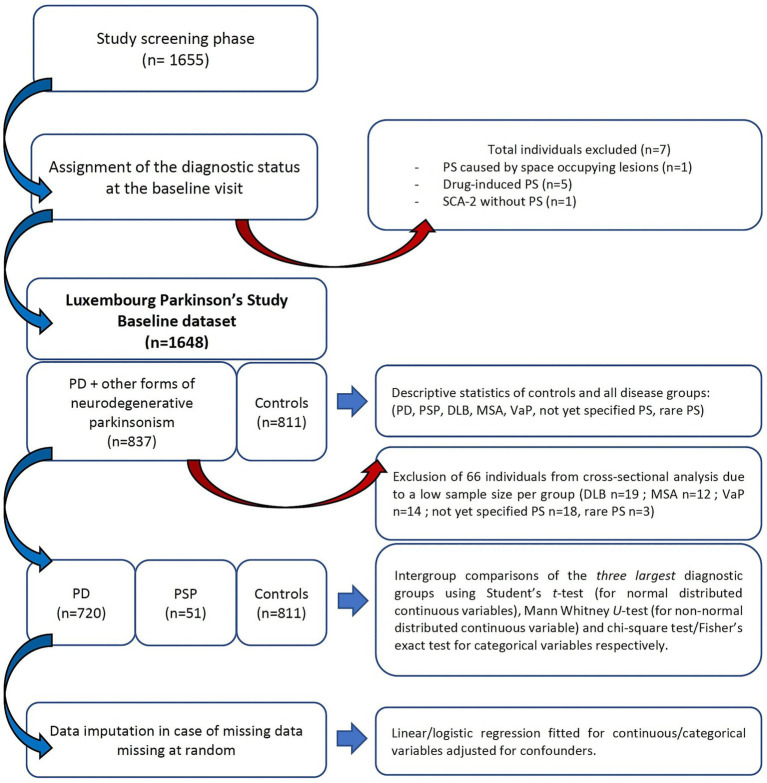
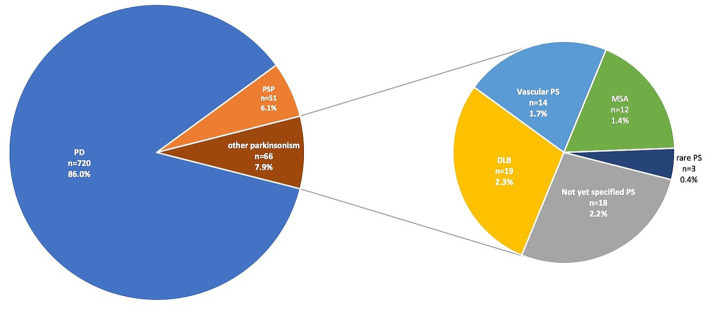
Methods: Epidemiological and clinical characteristics of all 1,648 participants divided in disease and control groups were investigated. Then, a cross-sectional group comparison was performed between the three largest groups: PD, progressive supranuclear palsy (PSP) and controls. Subsequently, multiple linear and logistic regression models were fitted adjusting for confounders.
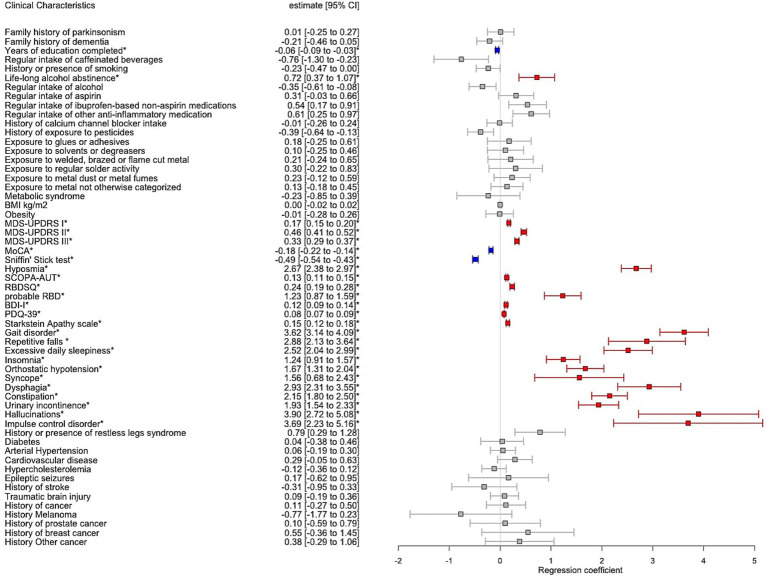
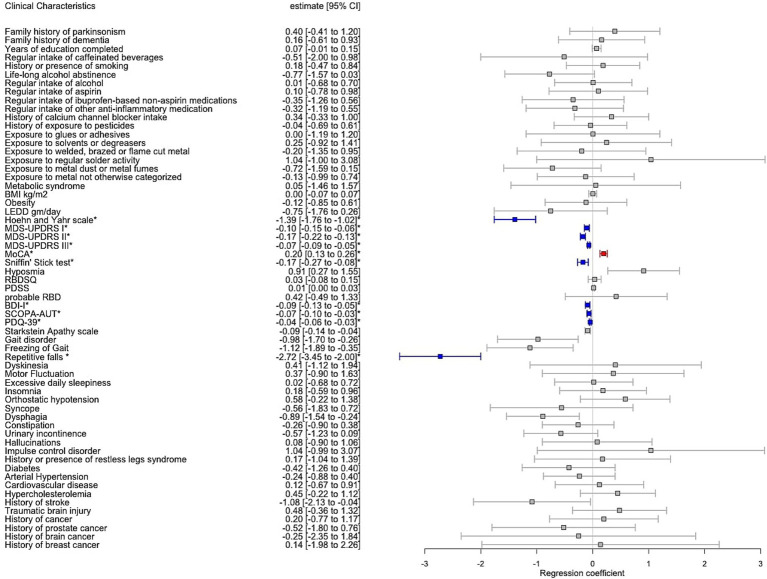
Results: The mean (SD) age at onset (AAO) of PD was 62.3 (11.8) years with 15% early onset (AAO < 50 years), mean disease duration 4.90 (5.16) years, male sex 66.5% and mean MDS-UPDRS III 35.2 (16.3). For PSP, the respective values were: 67.6 (8.2) years, all PSP with AAO > 50 years, 2.80 (2.62) years, 62.7% and 53.3 (19.5). The highest frequency of hyposmia was detected in PD followed by PSP and controls (72.9%; 53.2%; 14.7%), challenging the use of hyposmia as discriminating feature in PD vs. PSP. Alcohol abstinence was significantly higher in PD than controls (17.6 vs. 12.9%, p = 0.003).
Conclusion: Luxembourg Parkinson's study constitutes a valuable resource to strengthen the understanding of complex traits in the aforementioned neurodegenerative disorders. It corroborated several previously observed clinical profiles, and provided insight on frequency of hyposmia in PSP and dietary habits, such as alcohol abstinence in PD.Clinical trial registration: clinicaltrials.gov, NCT05266872.
Keywords: Parkinson’s disease; REM-sleep behaviour disorder; environment exposure; hyposmia; parkinsonian disorders; progressive supranuclear palsy.
Copyright © 2023 Pavelka, Rawal, Ghosh, Pauly, Pauly, Hanff, Kolber, Jónsdóttir, Mcintyre, Azaiz, Thiry, Vilasboas, Soboleva, Giraitis, Tsurkalenko, Sapienza, Diederich, Klucken, Glaab, Aguayo, Jubal, Perquin, Vaillant, May, Gantenbein, Satagopam, Krüger and on behalf of the NCER-PD Consortium.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous