

Preoperative sleep apnea screening protocol reduces medical emergency team activation in patients with atrial fibrillation
- PMID: 38174855
- PMCID: PMC11063713
- DOI: 10.5664/jcsm.11002
Preoperative sleep apnea screening protocol reduces medical emergency team activation in patients with atrial fibrillation
Abstract
Study objectives: The association of in-hospital medical emergency team activation (META) among patients with atrial fibrillation (AF) at risk for obstructive sleep apnea (OSA) is unclear. This study evaluates the performance of the DOISNORE50 sleep questionnaire as an OSA screener for patients with AF and determines the prevalence of META among perioperative patients with underlying AF who have a diagnosis or are at risk for OSA.
Methods: A prospective perioperative cohort of 2,926 patients with the diagnosis of AF was assessed for DOISNORE50 questionnaire screening. Propensity-score matching was used to match patients' physical characteristics, comorbidities, length of stay, and inpatient continuous positive airway pressure device usage. META and intensive care unit admissions during the surgical encounter, 30-day hospital readmissions, and 30-day emergency department visits were evaluated.
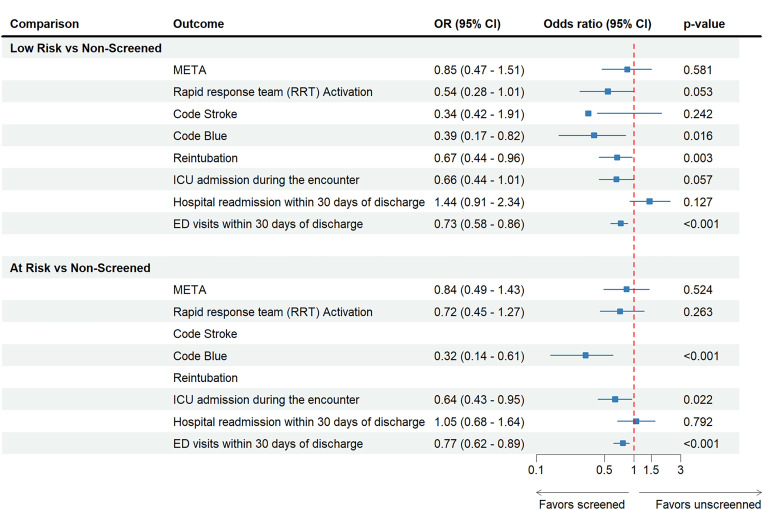
Results: A total of 1,509 out of 2,926 AF patients completed the DOISNORE50 questionnaire and were enrolled in the OSA safety protocol. Following propensity-score matching, there were reduced adjusted odds of META in the screened group of 0.69 (95% confidence interval: 0.48-0.98, P < .001) in comparison to the unscreened group. The adjusted odds of intensive care unit admissions and emergency department visits within 30 days of discharge were statistically lower for the screened group compared with the unscreened group.
Conclusions: Among perioperative AF patients, evidence supports DOISNORE50 screening and implementation of an OSA safety protocol for reduction of META. This study identified decreased odds of META, intensive care unit admissions, and emergency department visits among the screened group. The high-risk and known OSA group showed reduced odds of META following the implementation of an OSA safety protocol.
Citation: Saha AK, Sheehan KN, Xiang KR, et al. Preoperative sleep apnea screening protocol reduces medical emergency team activation in patients with atrial fibrillation. J Clin Sleep Med. 2024;20(5):783-792.
Keywords: DOISNORE50; OSA safety protocol; atrial fibrillation; complications; obstructive sleep apnea; perioperative.
© 2024 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have seen and approved the manuscript. The authors report no conflicts of interest.
Figures





References
-
- Veasey SC, Rosen IM . Obstructive sleep apnea in adults . N Engl J Med. 2019. ; 380 ( 15 ): 1442 – 1449 . - PubMed
-
- Fleming WE, Ferouz-Colborn A, Samoszuk MK, et al. . Blood biomarkers of endocrine, immune, inflammatory, and metabolic systems in obstructive sleep apnea . Clin Biochem. 2016. ; 49 ( 12 ): 854 – 861 . - PubMed
-
- Peppard PE, Young T, Palta M, Dempsey J, Skatrud J . Longitudinal study of moderate weight change and sleep-disordered breathing . JAMA. 2000. ; 284 ( 23 ): 3015 – 3021 . - PubMed
-
- Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V . Obstructive sleep apnea as a risk factor for stroke and death . N Engl J Med. 2005. ; 353 ( 19 ): 2034 – 2041 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
