

Interval cancer in the Córdoba Breast Tomosynthesis Screening Trial (CBTST): comparison of digital breast tomosynthesis plus digital mammography to digital mammography alone
- PMID: 38177619
- PMCID: PMC11255077
- DOI: 10.1007/s00330-023-10546-x
Interval cancer in the Córdoba Breast Tomosynthesis Screening Trial (CBTST): comparison of digital breast tomosynthesis plus digital mammography to digital mammography alone
Abstract
Purpose: This work aims to compare the interval cancer rate and interval cancer characteristics between women screened with digital breast tomosynthesis (DBT) + digital mammography (DM) and those screened with DM alone.
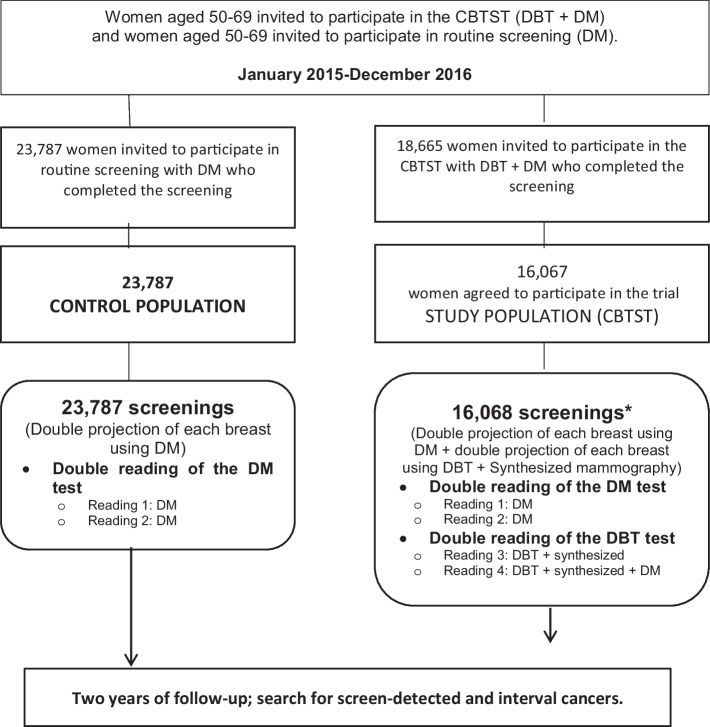
Methods: The interval cancer rate and interval cancer characteristics of the study population included in the Córdoba Breast Tomosynthesis Screening Trial (CBTST) were compared to a contemporary control population screened with DM. The tumour characteristics of screen-detected and interval cancers were also compared. Contingency tables were used to compare interval cancer rates. The chi-square test and Fisher's exact test were used to compare the qualitative characteristics of the cancers whereas Student's t test and the Mann-Whitney U test were used to analyse quantitative features.
Results: A total of 16,068 screening exams with DBT + DM were conducted within the CBTST (mean age 57.59 ± 5.9 [SD]) between January 2015 and December 2016 (study population). In parallel, 23,787 women (mean age 58.89 ± 5.9 standard deviation [SD]) were screened with DM (control population). The interval cancer rate was lower in the study population than in the control population (15 [0.93‰; 95% confidence interval (CI): 0.73, 1.14] vs 43 [1.8‰; 95% CI: 1.58, 2.04] respectively; p = 0.045). The difference in rate was more marked in women with dense breasts (0.95‰ in the study population vs 3.17‰ in the control population; p = 0.031). Interval cancers were smaller in the study population than in the control population (p = 0.031).
Conclusions: The interval cancer rate was lower in women screened with DBT + DM compared to those screened with DM alone. These differences were more pronounced in women with dense breasts.
Clinical relevance statement: Women screened using tomosynthesis and digital mammography had a lower rate of interval cancer than women screened with digital mammography, with the greatest difference in the interval cancer rate observed in women with dense breasts.
Key points: • The interval cancer rate was lower in the study population (digital breast tomosynthesis [DBT] + digital mammography [DM]) than in the control population (DM). • The difference in interval cancer rates was more pronounced in women with dense breasts. • Interval cancers were smaller in the study population (DBT + DM) than in the control population (DM).
Keywords: Breast neoplasms; Digital breast tomosynthesis; Mammography; Mass screening.
© 2024. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures

Comment in
-
Can digital breast tomosynthesis decrease interval cancers in a breast cancer screening program?Eur Radiol. 2024 Aug;34(8):5425-5426. doi: 10.1007/s00330-024-10635-5. Epub 2024 Feb 6. Eur Radiol. 2024. PMID: 38319429 No abstract available.
References
-
- Hubbard RA, Kerlikowske K, Flowers CI, Yankaskas BC, Zhu W, Miglioretti DL. Cumulative probability of false-positive recall or biopsy recommendation after 10 years of screening mammography: a cohort study. Ann Intern Med. 2011;155(8):481–492. doi: 10.7326/0003-4819-155-8-201110180-00004. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
