

Prediction of response to neoadjuvant chemo-immunotherapy in patients with esophageal squamous cell carcinoma by a rapid breath test
- PMID: 38177659
- PMCID: PMC10876947
- DOI: 10.1038/s41416-023-02547-w
Prediction of response to neoadjuvant chemo-immunotherapy in patients with esophageal squamous cell carcinoma by a rapid breath test
Abstract
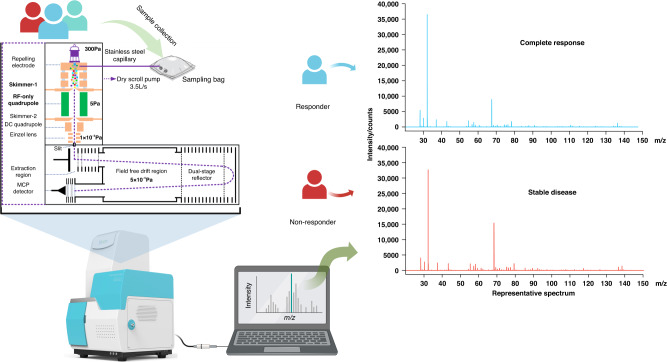
Background: Neoadjuvant chemo-immunotherapy combination has shown remarkable advances in the management of esophageal squamous cell carcinoma (ESCC). However, the identification of a reliable biomarker for predicting the response to this chemo-immunotherapy regimen remains elusive. While computed tomography (CT) is widely utilized for response evaluation, its inherent limitations in terms of accuracy are well recognized. Therefore, in this study, we present a novel technique to predict the response of ESCC patients before receiving chemo-immunotherapy by testing volatile organic compounds (VOCs) in exhaled breath.
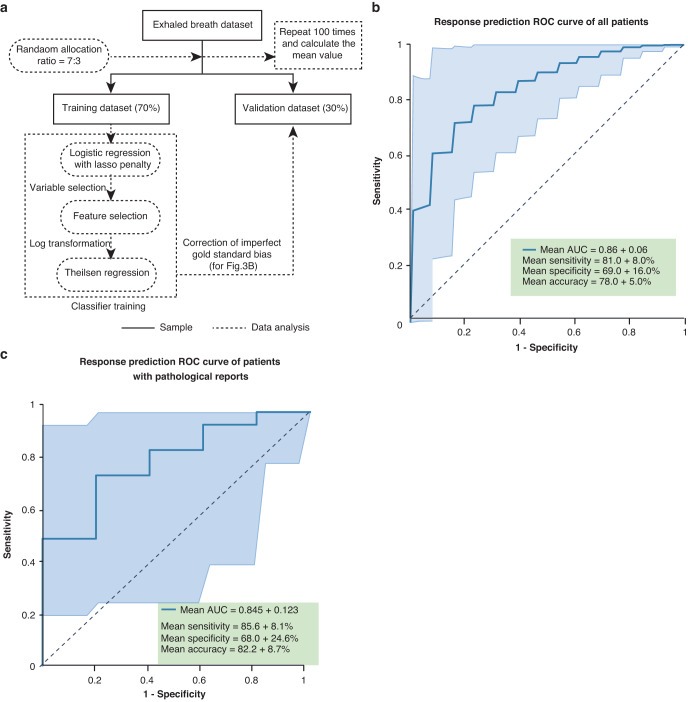
Methods: This study employed a prospective-specimen-collection, retrospective-blinded-evaluation design. Patients' baseline breath samples were collected and analyzed using high-pressure photon ionization time-of-flight mass spectrometry (HPPI-TOFMS). Subsequently, patients were categorized as responders or non-responders based on the evaluation of therapeutic response using pathology (for patients who underwent surgery) or CT images (for patients who did not receive surgery).
Results: A total of 133 patients were included in this study, with 91 responders who achieved either a complete response (CR) or a partial response (PR), and 42 non-responders who had stable disease (SD) or progressive disease (PD). Among 83 participants who underwent both evaluations with CT and pathology, the paired t-test revealed significant differences between the two methods (p < 0.05). For the breath test prediction model using breath test data from all participants, the validation set demonstrated mean area under the curve (AUC) of 0.86 ± 0.06. For 83 patients with pathological reports, the breath test achieved mean AUC of 0.845 ± 0.123.
Conclusions: Since CT has inherent weakness in hollow organ assessment and no other ideal biomarker has been found, our study provided a noninvasive, feasible, and inexpensive tool that could precisely predict ESCC patients' response to neoadjuvant chemo-immunotherapy combination using breath test based on HPPI-TOFMS.
© 2024. The Author(s), under exclusive licence to Springer Nature Limited.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Sun JM, Shen L, Shah MA, Enzinger P, Adenis A, Doi T, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet. 2021;398:759–71. doi: 10.1016/S0140-6736(21)01234-4. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
