

Estrogen receptor-negative/progesterone receptor-positive breast cancer has distinct characteristics and pathologic complete response rate after neoadjuvant chemotherapy
- PMID: 38178166
- PMCID: PMC10765627
- DOI: 10.1186/s13000-023-01433-6
Estrogen receptor-negative/progesterone receptor-positive breast cancer has distinct characteristics and pathologic complete response rate after neoadjuvant chemotherapy
Abstract
Purpose: The status of hormone receptors (HR) is an independent factor affecting survival and chemotherapy sensitivity in breast cancer (BC) patients, with estrogen receptor (ER) and progesterone receptor (PR) having the most significant effects. The ER-/PR + phenotype has been controversial in BC, and experts will face many challenges in determining treatment strategies. Herein, we systematically analyzed the clinicopathological characteristics of the ER-/PR + phenotype in BC patients and the response to chemotherapy.
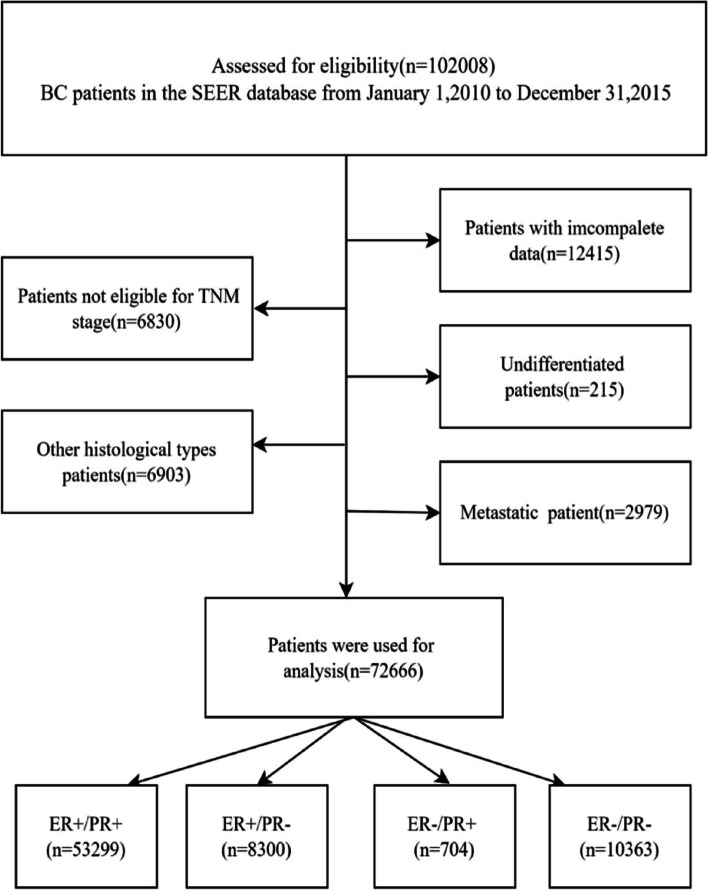
Patients and methods: We included two cohorts. The first cohort counted the relationship between clinicopathologic data and survival outcomes for 72,666 female patients in the Surveillance, Epidemiology, and End Results (SEER) database. The second cohort analyzed the relationship between clinicopathological data and pathologic complete response (pCR) rate in 879 patients at the Harbin Medical University Cancer Hospital. The classification data were compared by the chi-square test and Fister's exact test of the Logistic regression model, and predictor variables with P < 0.05 in the univariate analysis were included in the multivariate regression analysis. The Kaplan-Meier method evaluated breast cancer-specific survival (BCSS) and overall survival (OS) to investigate the relationship between different HR typing and survival and pCR.
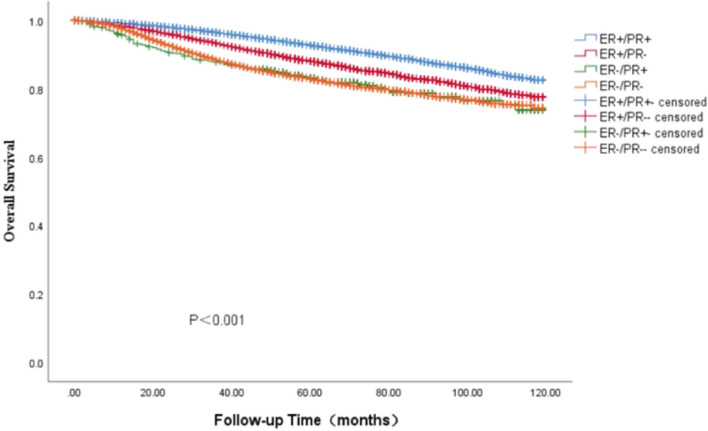
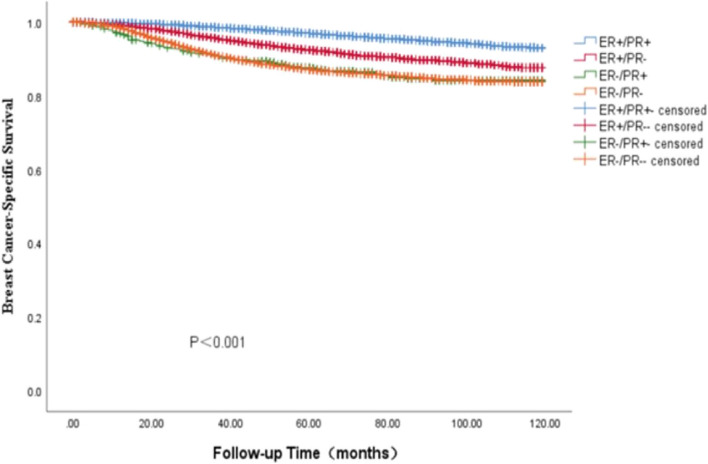
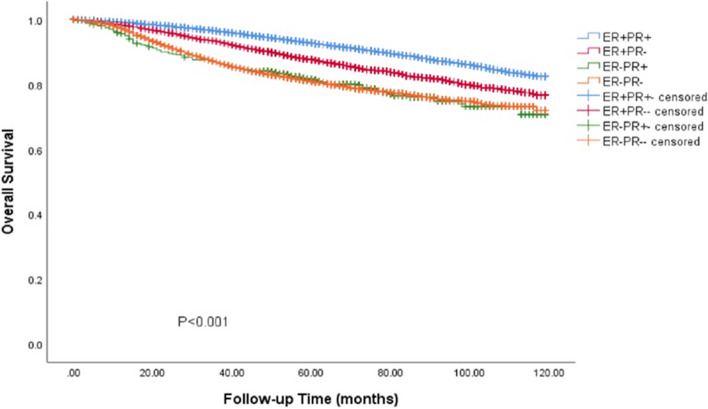
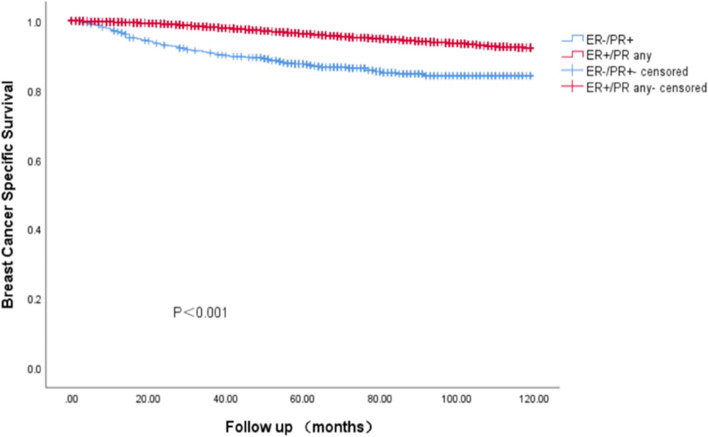
Results: In the two cohorts, 704 (0.9%) and 11 (1.3%) patients had the ER-/PR + phenotype, respectively. The clinicopathologic features of patients with the ER-/PR + phenotype are more similar to those of the ER-/PR- phenotype. The ER-/PR + phenotype is more common in younger and premenopausal women, and most ER-/PR + phenotypes exhibit higher histological grades. Survival analysis showed that there were significant differences in OS and BCSS among patients with different HR states (P < 0.001). The survival results of patients with the ER + /PR + phenotype were the best. The prognosis of the ER-/PR + phenotype was similar to that of the ER-/PR- phenotype. On the other hand, we found that HR status was also an independent predictor of post-NAC pCR rate in BC patients. The ER + /PR- and ER-/PR- phenotypes were more sensitive to chemotherapy than the ER + /PR + phenotypes.
Conclusion: HR status is the main factor affecting BC's survival outcome and pCR rate. Patients with the ER-/PR + phenotype possess more aggressive biological factors and can benefit significantly from chemotherapy. We need to pay more attention to this group and achieve individualized treatment, which will help us treat BC better and provide new targets and blueprints for our clinical treatment.
Keywords: Breast cancer; Estrogen receptor; Neoadjuvant chemotherapy; Pathologic complete response; Progesterone receptor.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
