

Influence of therapeutic plasma exchange treatment on short-term mortality of critically ill adult patients with sepsis-induced organ dysfunction: a systematic review and meta-analysis
- PMID: 38178170
- PMCID: PMC10768220
- DOI: 10.1186/s13054-023-04795-x
Influence of therapeutic plasma exchange treatment on short-term mortality of critically ill adult patients with sepsis-induced organ dysfunction: a systematic review and meta-analysis
Abstract
Introduction: The impact of therapeutic plasma exchange (TPE) on short-term mortality in adult patients with sepsis-induced organ dysfunction remains uncertain. The objective of the study is to assess the effect of adjunct TPE in this setting through a comprehensive literature review.
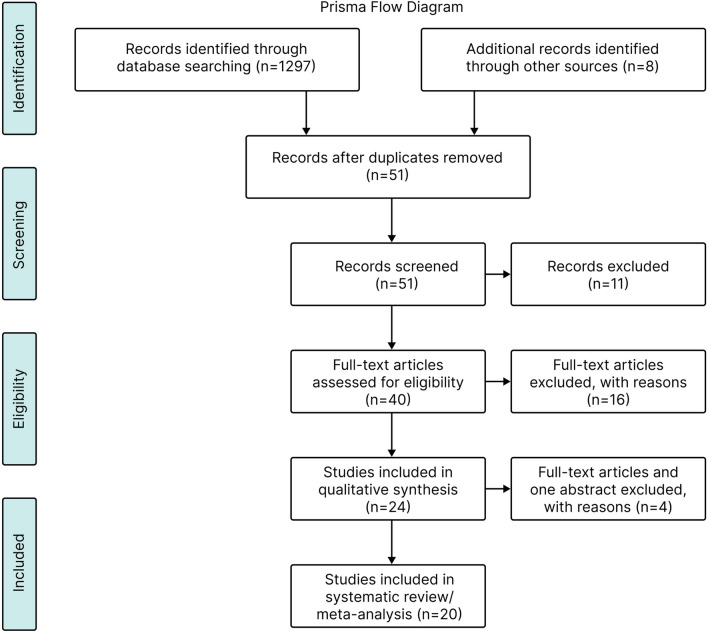
Methods: The National Library of Medicine's Medline, Ovid (Embase), the Cochrane Library database and clinicaltrial.gov from January 01, 1966, until October 01, 2022, were searched for terms: therapeutic plasma exchange, plasmapheresis, sepsis, and septic shock. We reviewed, selected and extracted data from relevant randomized clinical trials (RCTs) and matched cohort studies (MCSs) comparing short-term mortality in critically ill adult septic patients treated with standard therapy versus those receiving adjunct TPE. Risk of bias was assessed in the RCTs using Cochrane Collaboration tool and in MCSs using ROBINS-I tool. Summary statistics, risk ratios (RRs), and confidence intervals (CIs) were calculated using random effects model.
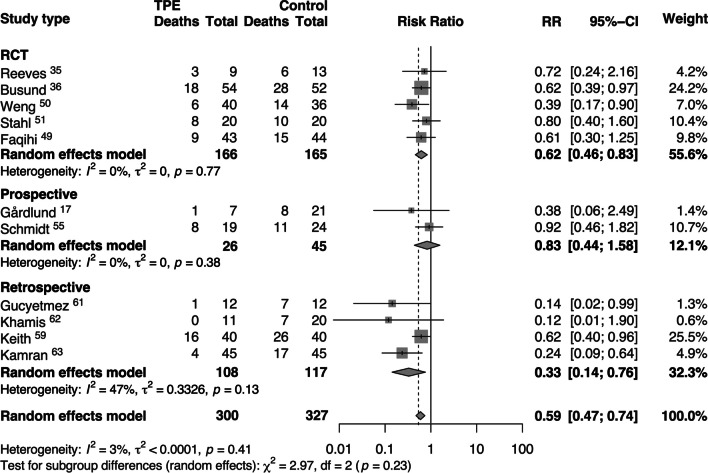
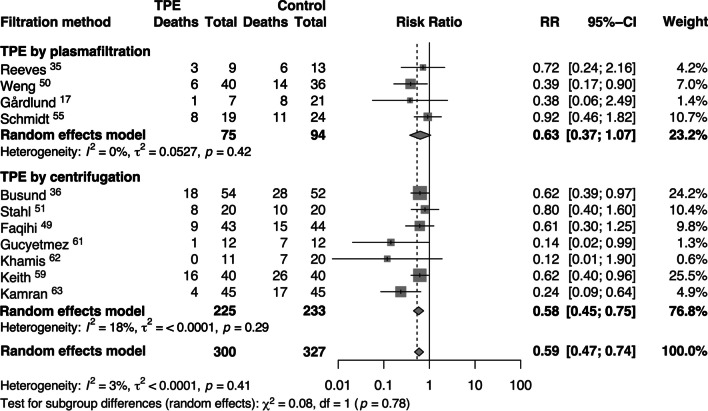
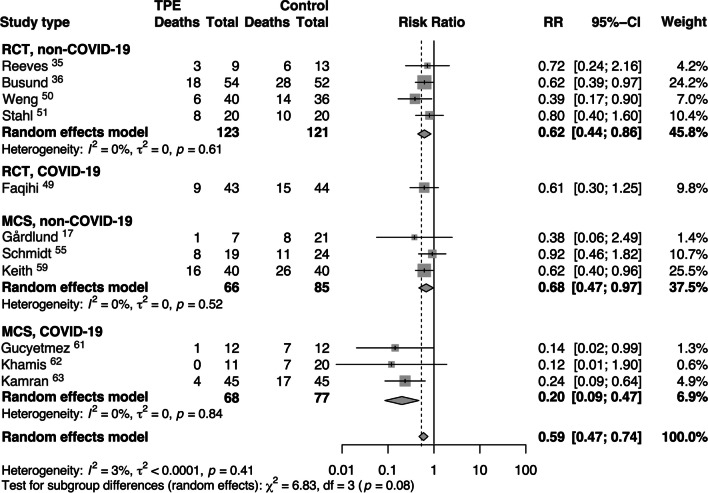
Results: This systematic review included 937 adult critically ill septic patients from five RCTs (n = 367) and fifteen MCSs (n = 570). Of these total, 543 received treatment with TPE in addition to standard care. The meta-analysis includes all five RCTs and only six MCSs (n = 627). The adjunct TPE treatment (n = 300) showed a significant reduction in short-term mortality (RR 0.59, 95% CI 0.47-0.74, I2 3%) compared to standard therapy alone (n = 327). The systematic review of all 20 trials revealed that adding TPE to the standard therapy of critically ill septic patients resulted in faster clinical and/or laboratory recovery.
Conclusions: Our comprehensive and up-to-date review demonstrates that adjunct TPE may provide potential survival benefits when compared to standard care for critically ill adult patients with sepsis-induced organ dysfunction. While results of this meta-analysis are encouraging, large well-designed randomized trials are required to identify the optimal patient population and TPE procedure characteristics prior to widespread adoption into practice.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The third international consensus definitions for sepsis and septic shock (sepsis-3) JAMA. 2016;315(8):801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
