

Hospitalisation patterns in interstitial lung diseases: data from the EXCITING-ILD registry
- PMID: 38178212
- PMCID: PMC10765927
- DOI: 10.1186/s12931-023-02588-y
Hospitalisation patterns in interstitial lung diseases: data from the EXCITING-ILD registry
Abstract
Background: Interstitial lung diseases (ILD) comprise a heterogeneous group of mainly chronic lung diseases with more than 200 entities and relevant differences in disease course and prognosis. Little data is available on hospitalisation patterns in ILD.
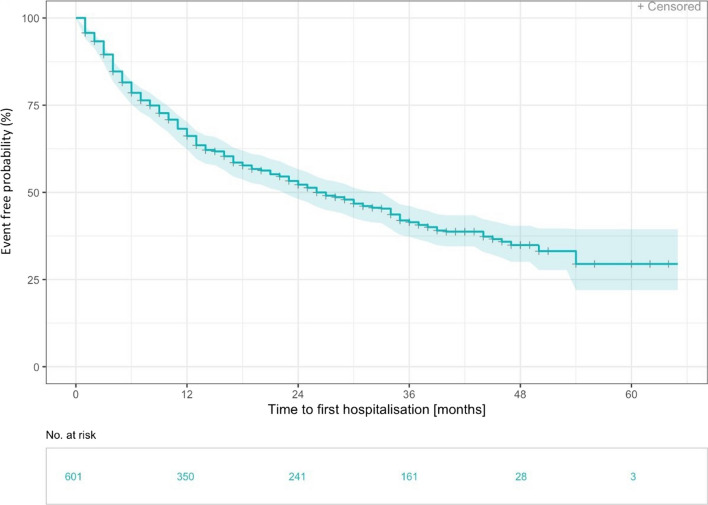
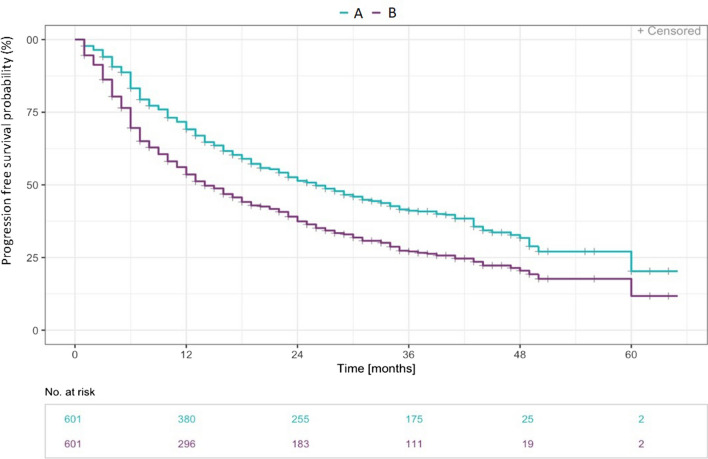
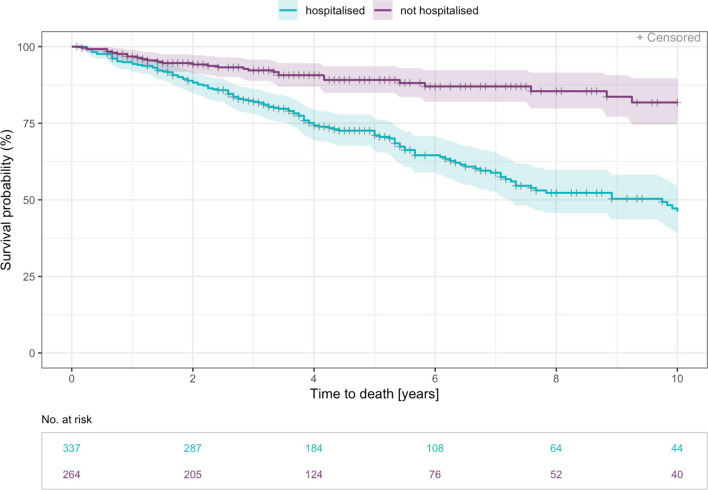
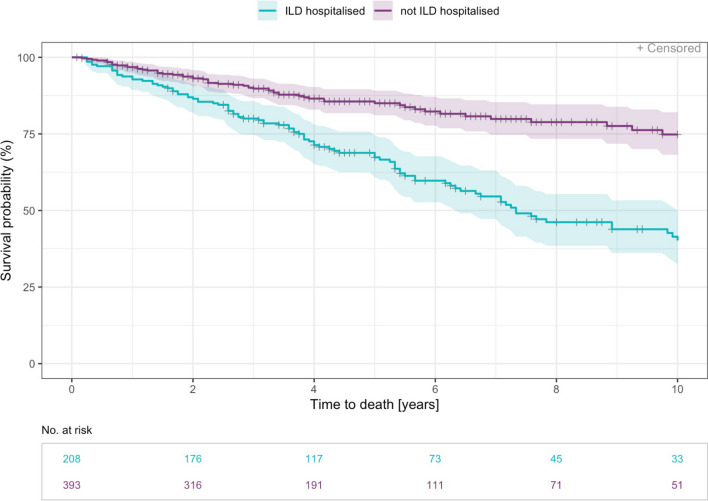
Methods: The EXCITING-ILD (Exploring Clinical and Epidemiological Characteristics of Interstitial Lung Diseases) registry was analysed for hospitalisations. Reasons for hospitalisation were classified as all cause, ILD-related and respiratory hospitalisations, and patients were analysed for frequency of hospitalisations, time to first non-elective hospitalisation, mortality and progression-free survival. Additionally, the risk for hospitalisation according to GAP index and ILD subtype was calculated by Cox proportional-hazard models as well as influencing factors on prediction of hospitalisation by logistic regression with forward selection.
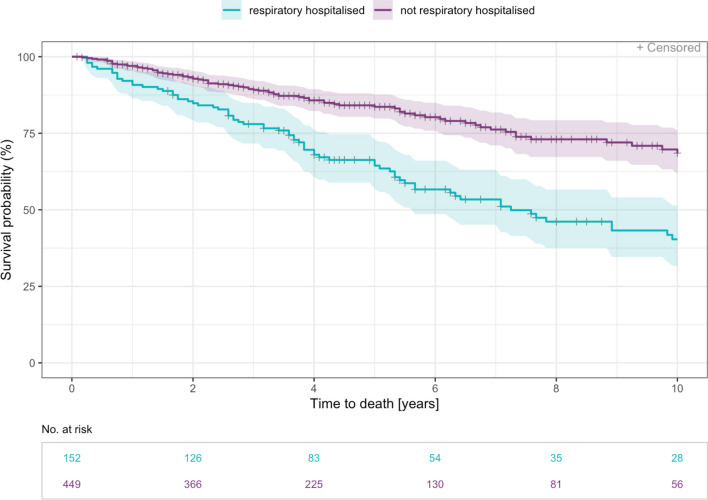
Results: In total, 601 patients were included. 1210 hospitalisations were recorded during the 6 months prior to registry inclusion until the last study visit. 800 (66.1%) were ILD-related, 59.3% of admissions were registered in the first year after inclusion. Mortality was associated with all cause, ILD-related and respiratory-related hospitalisation. Risk factors for hospitalisation were advanced disease (GAP Index stages II and III) and CTD (connective tissue disease)-ILDs. All cause hospitalisations were associated with pulmonary hypertension (OR 2.53, p = 0.005). ILD-related hospitalisations were associated with unclassifiable ILD and concomitant emphysema (OR = 2.133, p = 0.001) as well as with other granulomatous ILDs and a positive smoking status (OR = 3.082, p = 0.005).
Conclusion: Our results represent a crucial contribution in understanding predisposing factors for hospitalisation in ILD and its major impact on mortality. Further studies to characterize the most vulnerable patient group as well as approaches to prevent hospitalisations are warranted.
Keywords: Hospitalisation; ILD; IPF; Prognosis; Risk factors.
© 2023. The Author(s).
Conflict of interest statement
KB received payment for lectures from Boehringer Ingelheim and a grant from Sarkoidose-Netzwerk e.V. DS reports fees for lectures or consultations from AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Janssen, MSD, Sanofi, all outside the submitted work. CS reports fees for lectures GSK, AstraZeneca, Boehringer Ingelheim, Berlin Chemie. MJ reports fees for lectures or consultations from AstraZeneca, Bencard, Boehringer Ingelheim, GSK, HAL Allergy, Sanofi, all outside the submitted work. SV reports fees from Berlin Chemie, GSK, Lilly and Boehringer-Ingelheim. JB reports personal fees for lectures and consulting from Astra-Zeneca, Biogen, Boehringer-Ingelheim, BMS, Ferrer, Novartis, Roche, and Sanofi-Genzyme. MP has received payment or honoraria for lectures, presentations or educational events from Boehringer Ingelheim and AstraZeneca. VS received support for attending meetings from CSL Behring. PM received fees for consulting and lectures from Boehringer-Ingelheim and Roche. MK reports grants, consulting fees, and payment for lectures from Boehringer Ingelheim and Roche. All other authors have nothing to disclose.
Figures
References
-
- Valeyre D, Duchemann B, Annesi-Maesano I, et al. Interstitial lung diseases, in Respiratory Epidemiology, T. Welte, I. Annesi-Maesano, G. Viegi, and B. Lundbäck,Eds., vol. 65 of ERSMonograph, chapter 6, ERS, 2014.
-
- American Thoracic Society and European Respiratory Society American Thoracic Society/European Respiratory Society international multidisciplinary consensus classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2002;165(2):277–304. doi: 10.1164/ajrccm.165.2.ats01. - DOI - PubMed
-
- Travis WD, Costabel U, Hansell D. An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733–748. doi: 10.1164/rccm.201308-1483ST. - DOI - PMC - PubMed
-
- Raghu G, Remy-Jardin M, Richeldi L, Thomson CC, Inoue Y, Johkoh T, Kreuter M, Lynch DA, Maher TM, Martinez FJ, Molina-Molina M, Myers JL, Nicholson AG, Ryerson CJ, Strek ME, Troy LK, Wijsenbeek M, Mammen MJ, Hossain T, Bissell BD, Herman DD, Hon SM, Kheir F, Khor YH, Macrea M, Antoniou KM, Bouros D, Buendia-Roldan I, Caro F, Crestani B, Ho L, Morisset J, Olson AL, Podolanczuk A, Poletti V, Selman M, Ewing T, Jones S, Knight SL, Ghazipura M, Wilson KC. Idiopathic pulmonary fibrosis (an Update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2022;205(9):e18–e47. doi: 10.1164/rccm.202202-0399ST. - DOI - PMC - PubMed
-
- Khanna D, Lin CJF, Furst DE, Goldin J, Kim G, Kuwana M, Allanore Y, Matucci-Cerinic M, Distler O, Shima Y, van Laar JM, Spotswood H, Wagner B, Siegel J, Jahreis A, Denton CP, focuSSced investigators Tocilizumab in systemic sclerosis: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. 2020;8(10):963–974. doi: 10.1016/S2213-2600(20)30318-0. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
