

Implications of oral dysbiosis and HPV infection in head and neck cancer: from molecular and cellular mechanisms to early diagnosis and therapy
- PMID: 38179168
- PMCID: PMC10765588
- DOI: 10.3389/fonc.2023.1273516
Implications of oral dysbiosis and HPV infection in head and neck cancer: from molecular and cellular mechanisms to early diagnosis and therapy
Abstract
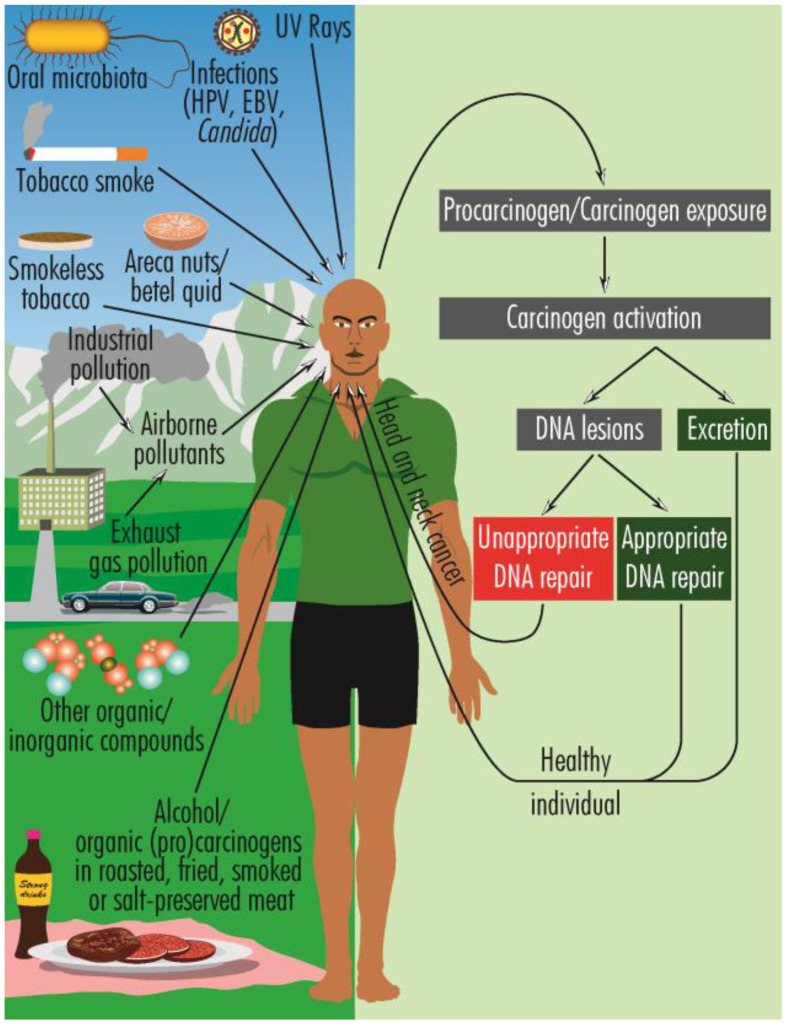
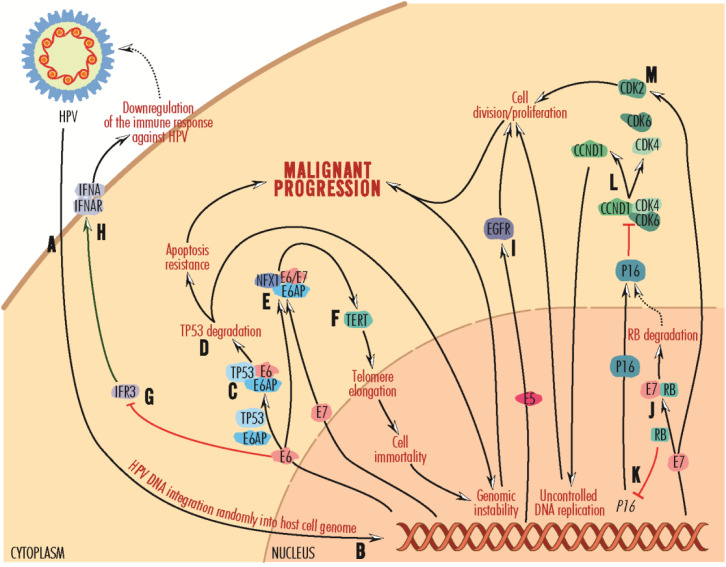
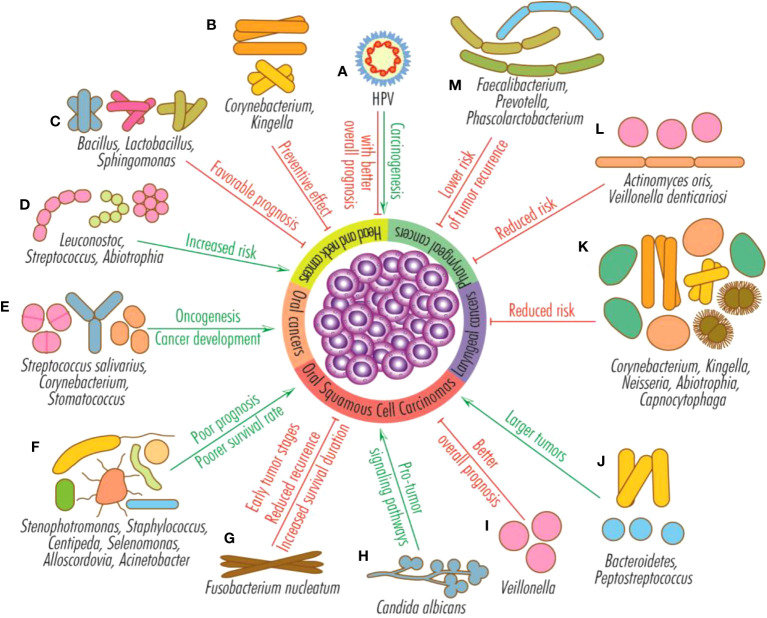
Head and neck cancer (HNC) is the sixth most common type of cancer, with more than half a million new cases annually. This review focuses on the role of oral dysbiosis and HPV infection in HNCs, presenting the involved taxons, molecular effectors and pathways, as well as the HPV-associated particularities of genetic and epigenetic changes and of the tumor microenvironment occurred in different stages of tumor development. Oral dysbiosis is associated with the evolution of HNCs, through multiple mechanisms such as inflammation, genotoxins release, modulation of the innate and acquired immune response, carcinogens and anticarcinogens production, generation of oxidative stress, induction of mutations. Thus, novel microbiome-derived biomarkers and interventions could significantly contribute to achieving the desideratum of personalized management of oncologic patients, regarding both early diagnosis and treatment. The results reported by different studies are not always congruent regarding the variations in the abundance of different taxons in HNCs. However, there is a consistent reporting of a higher abundance of Gram-negative species such as Fusobacterium, Leptotrichia, Treponema, Porphyromonas gingivalis, Prevotella, Bacteroidetes, Haemophilus, Veillonella, Pseudomonas, Enterobacterales, which are probably responsible of chronic inflammation and modulation of tumor microenvironment. Candida albicans is the dominant fungi found in oral carcinoma being also associated with shorter survival rate. Specific microbial signatures (e.g., F. nucleatum, Bacteroidetes and Peptostreptococcus) have been associated with later stages and larger tumor, suggesting their potential to be used as biomarkers for tumor stratification and prognosis. On the other hand, increased abundance of Corynebacterium, Kingella, Abiotrophia is associated with a reduced risk of HNC. Microbiome could also provide biomarkers for differentiating between oropharyngeal and hypopharyngeal cancers as well as between HPV-positive and HPV-negative tumors. Ongoing clinical trials aim to validate non-invasive tests for microbiome-derived biomarkers detection in oral and throat cancers, especially within high-risk populations. Oro-pharyngeal dysbiosis could also impact the HNCs therapy and associated side-effects of radiotherapy, chemotherapy, and immunotherapy. HPV-positive tumors harbor fewer mutations, as well as different DNA methylation pattern and tumor microenvironment. Therefore, elucidation of the molecular mechanisms by which oral microbiota and HPV infection influence the HNC initiation and progression, screening for HPV infection and vaccination against HPV, adopting a good oral hygiene, and preventing oral dysbiosis are important tools for advancing in the battle with this public health global challenge.
Keywords: HNC; HPV infection; oral microbiota; risk factors; signaling pathways; tumor microenvironment.
Copyright © 2023 Constantin, Chifiriuc, Mihaescu, Vrancianu, Dobre, Cristian, Bleotu, Bertesteanu, Grigore, Serban and Cirstoiu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources