

Left-Ventricular Unloading With Impella During Refractory Cardiac Arrest Treated With Extracorporeal Cardiopulmonary Resuscitation: A Systematic Review and Meta-Analysis
- PMID: 38180032
- PMCID: PMC10876179
- DOI: 10.1097/CCM.0000000000006157
Left-Ventricular Unloading With Impella During Refractory Cardiac Arrest Treated With Extracorporeal Cardiopulmonary Resuscitation: A Systematic Review and Meta-Analysis
Abstract
Objectives: Extracorporeal cardiopulmonary resuscitation (ECPR) is the implementation of venoarterial extracorporeal membrane oxygenation (VA-ECMO) during refractory cardiac arrest. The role of left-ventricular (LV) unloading with Impella in addition to VA-ECMO ("ECMELLA") remains unclear during ECPR. This is the first systematic review and meta-analysis to characterize patients with ECPR receiving LV unloading and to compare in-hospital mortality between ECMELLA and VA-ECMO during ECPR.
Data sources: Medline, Cochrane Central Register of Controlled Trials, Embase, and abstract websites of the three largest cardiology societies (American Heart Association, American College of Cardiology, and European Society of Cardiology).
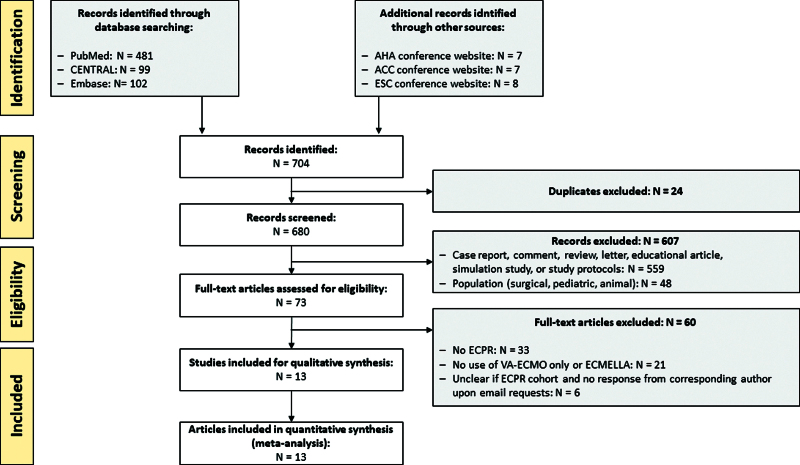
Study selection: Observational studies with adult patients with refractory cardiac arrest receiving ECPR with ECMELLA or VA-ECMO until July 2023 according to the Preferred Reported Items for Systematic Reviews and Meta-Analysis checklist.
Data extraction: Patient and treatment characteristics and in-hospital mortality from 13 study records at 32 hospitals with a total of 1014 ECPR patients. Odds ratios (ORs) and 95% CI were computed with the Mantel-Haenszel test using a random-effects model.
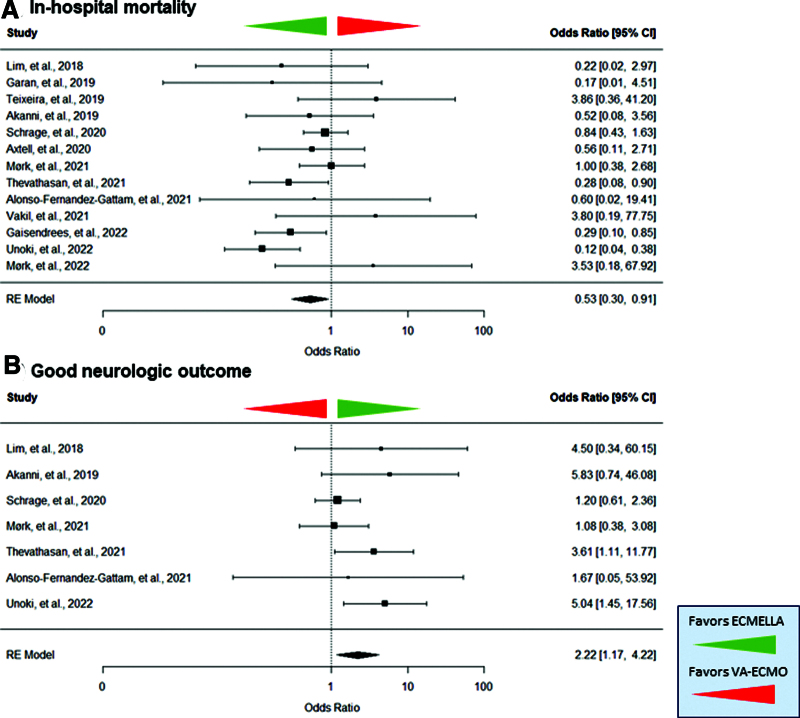
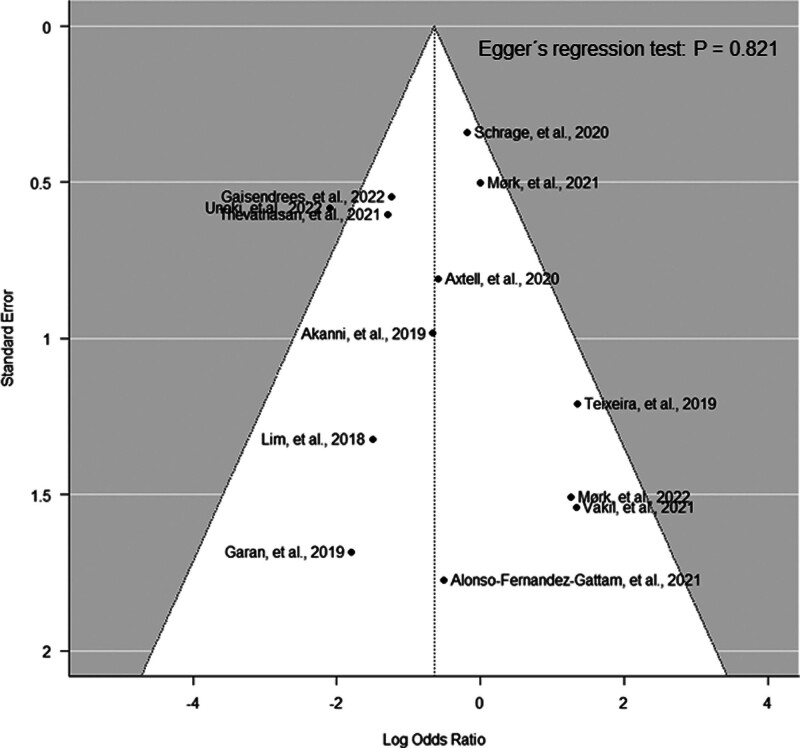
Data synthesis: Seven hundred sixty-two patients (75.1%) received VA-ECMO and 252 (24.9%) ECMELLA. Compared with VA-ECMO, the ECMELLA group was comprised of more patients with initial shockable electrocardiogram rhythms (58.6% vs. 49.3%), acute myocardial infarctions (79.7% vs. 51.5%), and percutaneous coronary interventions (79.0% vs. 47.5%). VA-ECMO alone was more frequently used in pulmonary embolism (9.5% vs. 0.7%). Age, rate of out-of-hospital cardiac arrest, and low-flow times were similar between both groups. ECMELLA support was associated with reduced odds of mortality (OR, 0.53 [95% CI, 0.30-0.91]) and higher odds of good neurologic outcome (OR, 2.22 [95% CI, 1.17-4.22]) compared with VA-ECMO support alone. ECMELLA therapy was associated with numerically increased but not significantly higher complication rates. Primary results remained robust in multiple sensitivity analyses.
Conclusions: ECMELLA support was predominantly used in patients with acute myocardial infarction and VA-ECMO for pulmonary embolism. ECMELLA support during ECPR might be associated with improved survival and neurologic outcome despite higher complication rates. However, indications and frequency of ECMELLA support varied strongly between institutions. Further scientific evidence is urgently required to elaborate standardized guidelines for the use of LV unloading during ECPR.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Drs. Schrage and Garan received funding from Abiomed. Dr. Schrage received funding from Abbott and AstraZeneca. Dr. Westermann received grants for honorary talks from AstraZeneca, Abiomed, Bayer, Boehringer Ingelheim, Edwards, Novartis, and Medtronic. Dr. Gregers received funding from the Odense University Hospital, Rigshospitalet’s Common Research Foundation, Novo Nordisk Foundation, and Beckett Foundation. Dr. Alonso-Fernandez-Gatta received funding from Instituto de Salud Carlos III (CM19/00055). Dr. Garan received funding from NuPulseCV and Maquet; he received support for article research from Abbott. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Mechanical Left-Ventricular Unloading in Extracorporeal Cardiopulmonary Resuscitation: A State of Clinical Equipoise.Crit Care Med. 2024 Mar 1;52(3):512-515. doi: 10.1097/CCM.0000000000006179. Epub 2024 Feb 21. Crit Care Med. 2024. PMID: 38381015 No abstract available.
References
-
- Belohlavek J, Smalcova J, Rob D, et al. ; Prague OHCA Study Group: Effect of intra-arrest transport, extracorporeal cardiopulmonary resuscitation, and immediate invasive assessment and treatment on functional neurologic outcome in refractory out-of-hospital cardiac arrest: A randomized clinical trial. JAMA. 2022; 327:737–747 - PMC - PubMed
-
- Suverein MM, Delnoij TSR, Lorusso R, et al. : Early extracorporeal CPR for refractory out-of-hospital cardiac arrest. N Engl J Med. 2023; 388:299–309 - PubMed
-
- Low CJW, Ramanathan K, Ling RR, et al. : Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with cardiac arrest: A comparative meta-analysis and trial sequential analysis. Lancet Respir Med. 2023; 11:883–893 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
