

Prognostic model for survival in patients with neuroendocrine carcinomas of the cervix: SEER database analysis and a single-center retrospective study
- PMID: 38181016
- PMCID: PMC10769015
- DOI: 10.1371/journal.pone.0296446
Prognostic model for survival in patients with neuroendocrine carcinomas of the cervix: SEER database analysis and a single-center retrospective study
Abstract
Objective: Neuroendocrine carcinoma of the cervix (NECC) is extremely rare in clinical practice. This study aimed to methodologically analyze the clinicopathological factors associated with NECC patients and to develop a validated survival prediction model.
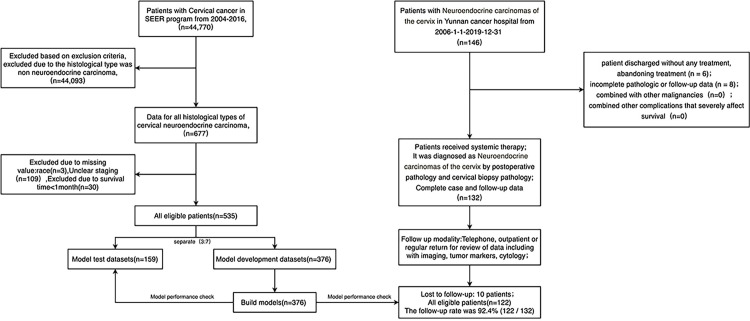
Methods: A total of 535 patients diagnosed with NECC between 2004 and 2016 were identified from the Surveillance, Epidemiology and End Results (SEER) database, while 122 patients diagnosed with NECC at Yunnan Cancer Hospital (YCH) from 2006 to 2019 were also recruited. Patients from the SEER database were divided into a training cohort (n = 376) and a validation cohort (n = 159) in a 7:3 ratio for the construction and internal validation of the nomogram. External validation was performed in a cohort at YCH. The Kaplan-Meier method was used for survival analysis, the Log-rank method test was used for univariate analysis of prognostic influences, and the Cox regression model was used for multivariate analysis.
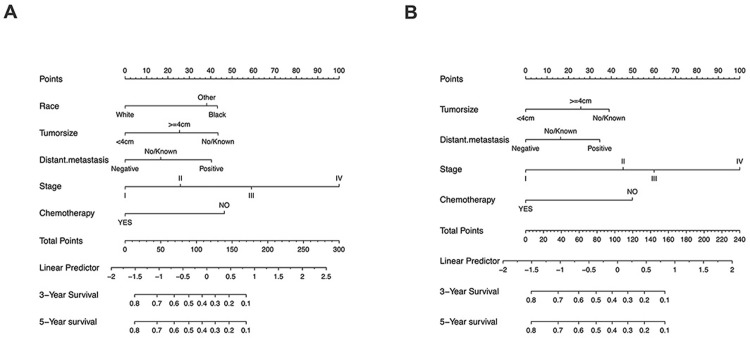
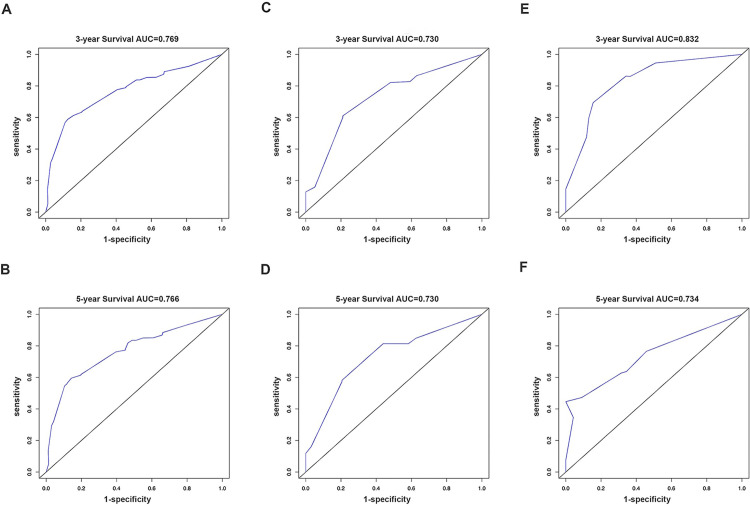
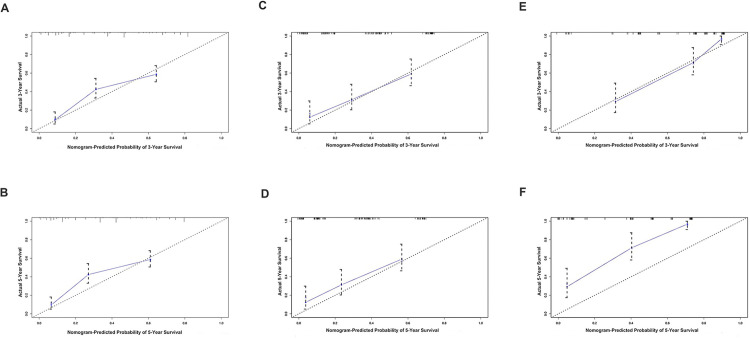
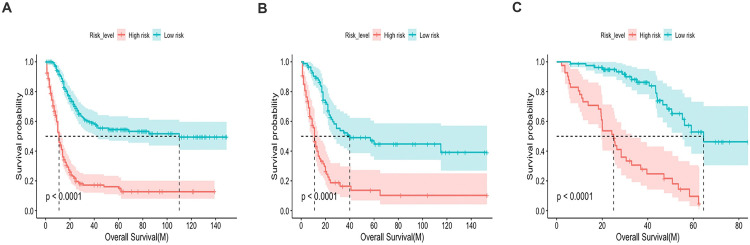
Results: The 3-year and 5-year overall survival (OS) rates for patients with NECC in SEER were 43.6% and 39.7%, respectively. In the training cohort, multivariate analysis showed independent prognostic factors for NECC patients including race, tumor size, distant metastasis, stage, and chemotherapy (p<0.05). For extended application in other cohorts, a nomogram including four factors without race was subsequently created. The consistency index (C-index) of the nomogram predicting survival was 0.736, which was well-validated in the validation cohorts (0.746 for the internal validation cohort and 0.765 for the external validation cohort). In both the training and validation cohorts, the 3-year survival rates predicted by the nomogram were comparable to the actual ones. We then succeeded in dividing patients with NECC into high- and low-risk groups concerning OS using the nomogram we developed. Besides, univariate analysis showed that chemotherapy ≥4 cycles may improve the OS of patients at YCH with NECC.
Conclusion: We successfully constructed a nomogram that precisely predicts the OS for patients with NECC based on the SEER database and a large single-center retrospective cohort. The visualized and practical model can distinguish high-risk patients for recurrence and death who may benefit from clinical trials of boost therapy effectively. We also found that patients who received more than 4 cycles of chemotherapy acquired survival benefits than those who received less than 4 cycles.
Copyright: © 2024 Yu et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Causes of death analysis and the prognostic model construction in neuroendocrine carcinoma of the cervix: A SEER-based study.Cancer Med. 2024 Aug;13(15):e70066. doi: 10.1002/cam4.70066. Cancer Med. 2024. PMID: 39118477 Free PMC article.
-
A nomogram for predicting prognosis for young cervical neuroendocrine carcinoma: A SEER-based study and external validation.Front Oncol. 2025 Jan 31;15:1463422. doi: 10.3389/fonc.2025.1463422. eCollection 2025. Front Oncol. 2025. PMID: 39959660 Free PMC article.
-
Competing risk nomogram and risk classification system for evaluating overall and cancer-specific survival in neuroendocrine carcinoma of the cervix: a population-based retrospective study.J Endocrinol Invest. 2024 Jun;47(6):1545-1557. doi: 10.1007/s40618-023-02261-7. Epub 2024 Jan 3. J Endocrinol Invest. 2024. PMID: 38170396 Free PMC article.
-
Construction and validation of the prognostic model for patients with neuroendocrine cervical carcinoma: a competing risk nomogram analysis.BMC Cancer. 2022 Jan 3;22(1):4. doi: 10.1186/s12885-021-09104-9. BMC Cancer. 2022. PMID: 34980030 Free PMC article.
-
Neuroendocrine carcinoma of the cervix: a systematic review of the literature.BMC Cancer. 2018 May 4;18(1):530. doi: 10.1186/s12885-018-4447-x. BMC Cancer. 2018. PMID: 29728073 Free PMC article.
Cited by
-
Radiotherapy can improve overall survival in patients with lymph-node positive, high-grade neuroendocrine cervical cancer: construction of two prognostic nomograms to predict treatment outcome.Front Oncol. 2024 Sep 13;14:1450382. doi: 10.3389/fonc.2024.1450382. eCollection 2024. Front Oncol. 2024. PMID: 39346736 Free PMC article.
-
Causes of death analysis and the prognostic model construction in neuroendocrine carcinoma of the cervix: A SEER-based study.Cancer Med. 2024 Aug;13(15):e70066. doi: 10.1002/cam4.70066. Cancer Med. 2024. PMID: 39118477 Free PMC article.
-
Total hysterectomy versus radical hysterectomy in neuroendocrine cervical cancer: a SEER-database analysis.J Cancer Res Clin Oncol. 2024 May 6;150(5):236. doi: 10.1007/s00432-024-05773-8. J Cancer Res Clin Oncol. 2024. PMID: 38710946 Free PMC article.
-
Exceptional response to trastuzumab deruxtecan in recurrent neuroendocrine cervical cancer: A case report.Gynecol Oncol Rep. 2025 Jun 26;60:101798. doi: 10.1016/j.gore.2025.101798. eCollection 2025 Aug. Gynecol Oncol Rep. 2025. PMID: 40678579 Free PMC article.
References
-
- Frumovitz M. Small- and Large-Cell Neuroendocrine Cervical Cancer. Oncology (Williston Park). 2016;30(1):70, 7–8, 93. . - PubMed
-
- Chen J, Sun Y, Chen L, Zang L, Lin C, Lu Y, et al.. Prognostic factors and treatment of neuroendocrine tumors of the uterine cervix based on the FIGO 2018 staging system: a single-institution study of 172 patients. PeerJ. 2021;9:e11563. Epub 20210706. doi: 10.7717/peerj.11563 ; PubMed Central PMCID: PMC8269661. - DOI - PMC - PubMed
