

Applying the EHA/EBMT grading for ICAHT after CAR-T: comparative incidence and association with infections and mortality
- PMID: 38181508
- PMCID: PMC11007437
- DOI: 10.1182/bloodadvances.2023011767
Applying the EHA/EBMT grading for ICAHT after CAR-T: comparative incidence and association with infections and mortality
Abstract
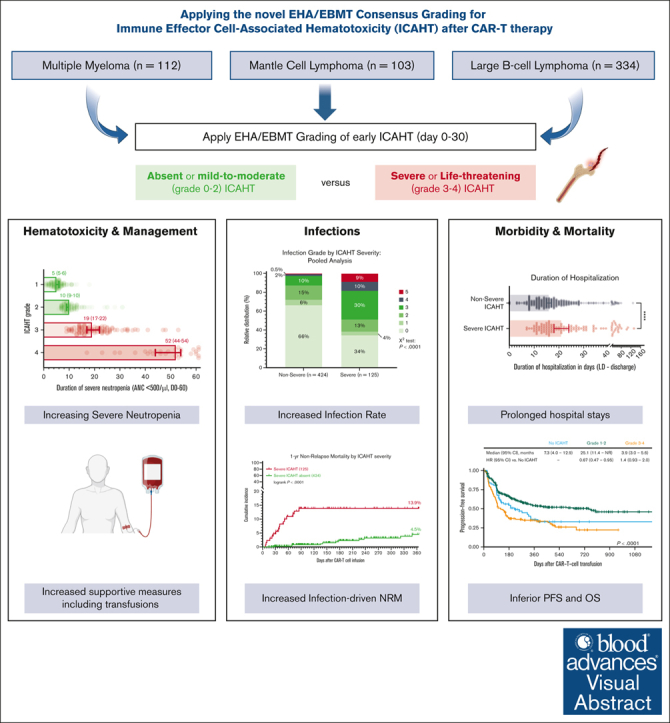
Cytopenias represent the most common side effect of CAR T-cell therapy (CAR-T) and can predispose for severe infectious complications. Current grading systems, such as the Common Terminology Criteria for Adverse Events (CTCAE), neither reflect the unique quality of post-CAR-T neutrophil recovery, nor do they reflect the inherent risk of infections due to protracted neutropenia. For this reason, a novel EHA/EBMT consensus grading was recently developed for Immune Effector Cell-Associated HematoToxicity (ICAHT). In this multicenter, observational study, we applied the grading system to a large real-world cohort of 549 patients treated with BCMA- or CD19-directed CAR-T for refractory B-cell malignancies (112 multiple myeloma [MM], 334 large B-cell lymphoma [LBCL], 103 mantle cell lymphoma [MCL]) and examined the clinical sequelae of severe (≥3°) ICAHT. The ICAHT grading was strongly associated with the cumulative duration of severe neutropenia (r = 0.92, P < .0001), the presence of multilineage cytopenias, and the use of platelet and red blood cell transfusions. We noted an increased rate of severe ICAHT in patients with MCL vs those with LBCL and MM (28% vs 23% vs 15%). Severe ICAHT was associated with a higher rate of severe infections (49% vs 13%, P < .0001), increased nonrelapse mortality (14% vs 4%, P < .0001), and inferior survival outcomes (1-year progression-free survival: 35% vs 51%, 1-year overall survival: 52% vs 73%, both P < .0001). Importantly, the ICAHT grading demonstrated superior capacity to predict severe infections compared with the CTCAE grading (c-index 0.73 vs 0.55, P < .0001 vs nonsignificant). Taken together, these data highlight the clinical relevance of the novel grading system and support the reporting of ICAHT severity in clinical trials evaluating CAR-T therapies.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: K.R. reports research funding, advisory, honoraria and travel support from Kite/Gilead; honoraria from Novartis; consultancy, honoraria from Bristol Myers Squibb (BMS)/Celgene; and travel support from Pierre Fabre. Y.W. reports research funding (to institution) from Incyte, InnoCare, LOXO Oncology, Eli Lilly, MorphoSys, Novartis, Genentech, and Genmab; advisory board (compensation to institution) from Eli Lilly, LOXO Oncology, TG Therapeutics, Incyte, InnoCare, Kite, Jansen, BeiGene, and AstraZeneca; consultancy (compensation to institution) from InnoCare and AbbVie; and honorarium (to institution) from Kite/Gilead. D.K.H. reports consulting or advisory role and research funding from BMS; and research funding from Adaptive Biotech. G.I. reports honoraria and travel support from Novartis, Kite/Gilead, BMS, AbbVie, Autolus, Sandoz, Miltenyi, and AstraZeneca. E.B. reports consultancy/honoraria from Novartis, Kite/Gilead, Roche, Takeda, and Incyte; research funding (paid to institution) from Amgen; and travel and personal fees from Roche and Incyte. O.P. has received honoraria or travel support from Astellas, Gilead, Jazz, MSD, Neovii Biotech, Novartis, Pfizer and Therakos. He has received research support from Gilead, Incyte, Jazz, Neovii Biotech and Takeda. He is a member of advisory boards to Jazz, Gilead, MSD, Omeros, Priothera, Shionogi and SOBI. F.M. reports travel support, advisory/honoraria from Novartis/Kite Gilead. W.B. reports consulting for and received honoraria from Novartis, Gilead; and consulting for and research funding from Miltenyi. J.M reports consulting for Pharmacyclics/AbbVie, Bayer, Gilead/Kite, BeiGene, Pfizer, Janssen, Celgene/BMS, Kyowa, Alexion, Fosun Kite, Seattle Genetics, Karyopharm, Aurobindo, Verastem, Genmab, Genentech/Roche, ADC Therapeutics, Epizyme, BeiGene, Novartis, MorphoSys/Incyte, MEI, TG Therapeutics, AstraZeneca, and Eli Lilly; research funding from Bayer, Gilead/Kite, Celgene, Merck, Portola, Incyte, Genentech, Pharmacyclics, Seattle Genetics, Janssen, Millennium, Novartis, BeiGene; and honoraria from Targeted Oncology, OncView, Curio, Physicians' Education Resource, and Seattle Genetics. V.L.B. received honoraria from Amgen, Pfizer, Kite/Gilead; research funding from Celgene, Kite/Gilead; honoraria from Kite/Gilead; Novartis; and served in a consultancy/advisory at Novartis, BMS, and Takeda. P.B. reports advisory role at Allogene, Amgen, BMS/Celgene, Kite/Gilead, Incyte, Novartis, and Pierre Fabre; consultancy at Jazz Pharmaceuticals, Miltenyi Biomedicine, Nektar, Novartis, and Pierre Fabre. F.L.L. has a scientific advisory role with A2, Allogene, Amgen, bluebird bio, BMS/Celgene, Calibr, Caribou, Cellular Biomedicine Group, Cowen, Daiichi Sankyo, EcoR1, Emerging Therapy Solutions, GammaDelta Therapeutics, Gerson Lehrman Group, Iovance, Kite Pharma, Janssen, Legend Biotech, Novartis, Sana, Takeda, Wugen, and Umoja; receives research support from Kite/Gilead, Novartis, BMS, 2seventy Bio, and Allogene; and reports that his institution holds unlicensed patents in his name in the field of cellular immunotherapy. Y.L. received research funding from Kite/Gilead, BMS, Janssen, Merck, Takeda, and 2seventy Bio; has consultancy/advisory role at Novartis, BMS, Janssen, Gamida Cells, NexImmune, NekTar Biotherapeutics, Pfizer, and Kite/Gilead; is on the data and safety monitoring board of Pfizer and Sorrento; and reports that all funds were to institution, no personal compensation. M.D.J. reports consultancy/advisory for Kite/Gilead and Myeloid Therapeutics; and research funding from Kite/Gilead, Incyte, and Loxo@Lilly. M.S. receives industry research support from Amgen, BMS/Celgene, Gilead, Janssen, Miltenyi Biotec, Novartis, Roche, Seattle Genetics, and Takeda; serves as a consultant/advisor to AvenCell, CDR-Life, Ichnos Sciences, Incyte Biosciences, Janssen, Miltenyi Biotec, Molecular Partners, Novartis, Pfizer; and Takeda; and serves on the speakers’ bureau at Amgen, AstraZeneca, BMS/Celgene, Gilead, GSK, Janssen, Novartis, Pfizer, Roche, and Takeda. None of the mentioned conflicts of interest were related to financing of the content of this manuscript. The remaining authors declare no competing financial interests.
Figures






References
-
- Locke FL, Miklos DB, Jacobson CA, et al. Axicabtagene Ciloleucel as second-line therapy for Large B-cell lymphoma. N Engl J Med. 2022;386(7):640–654. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
