

Automatic muscle impedance and nerve analyzer (AMINA) as a novel approach for classifying bioimpedance signals in intraoperative pelvic neuromonitoring
- PMID: 38182695
- PMCID: PMC10770322
- DOI: 10.1038/s41598-023-50504-7
Automatic muscle impedance and nerve analyzer (AMINA) as a novel approach for classifying bioimpedance signals in intraoperative pelvic neuromonitoring
Abstract
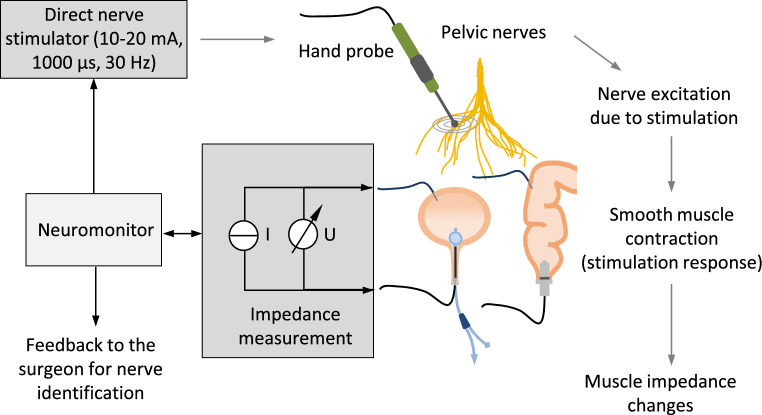
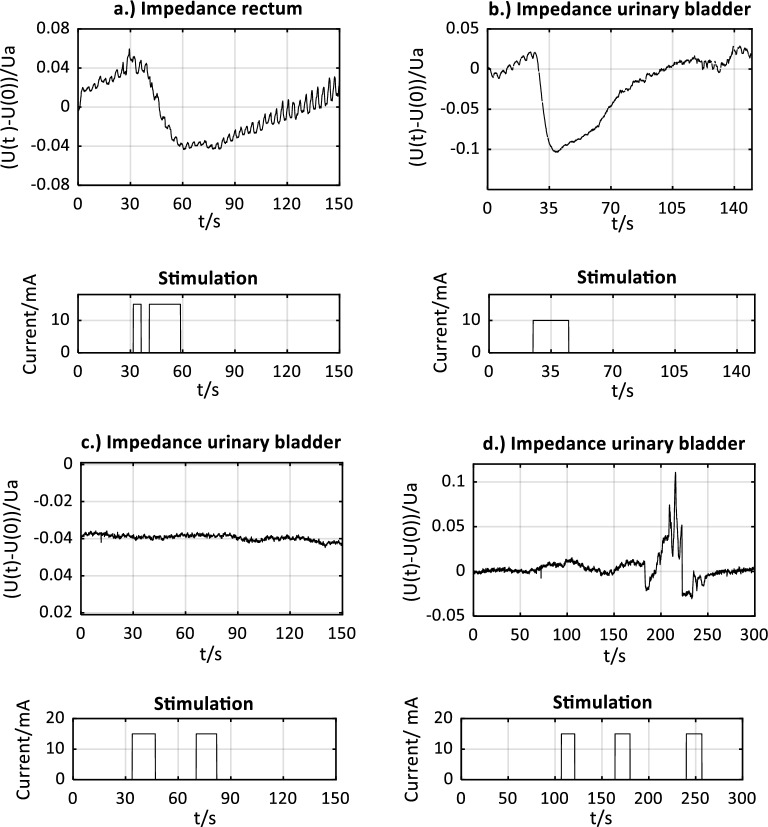
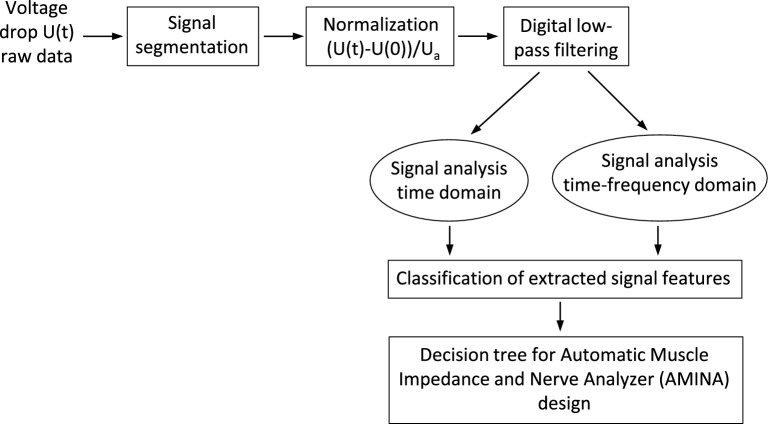
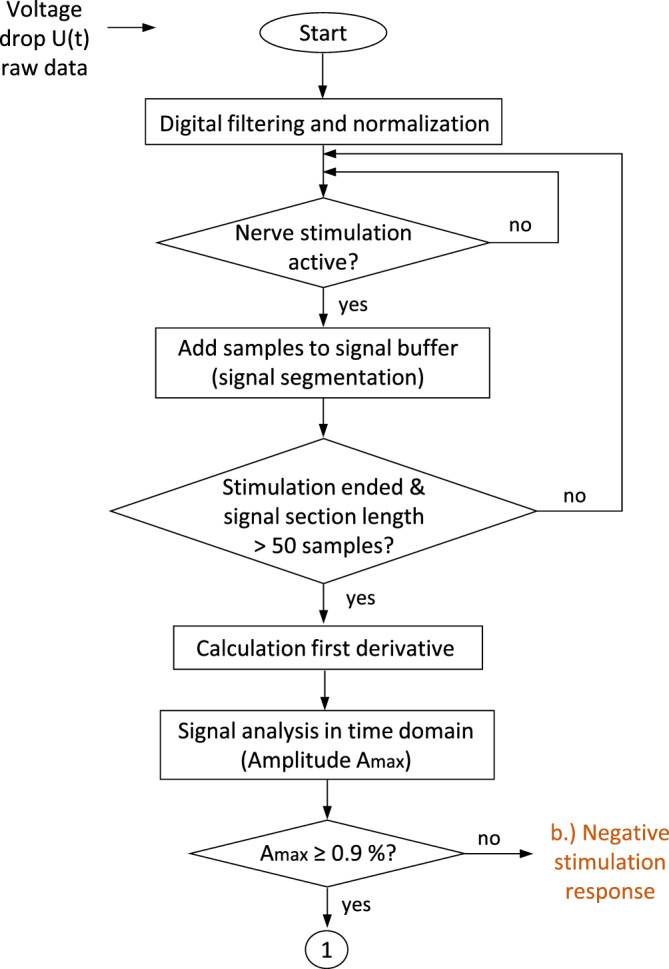
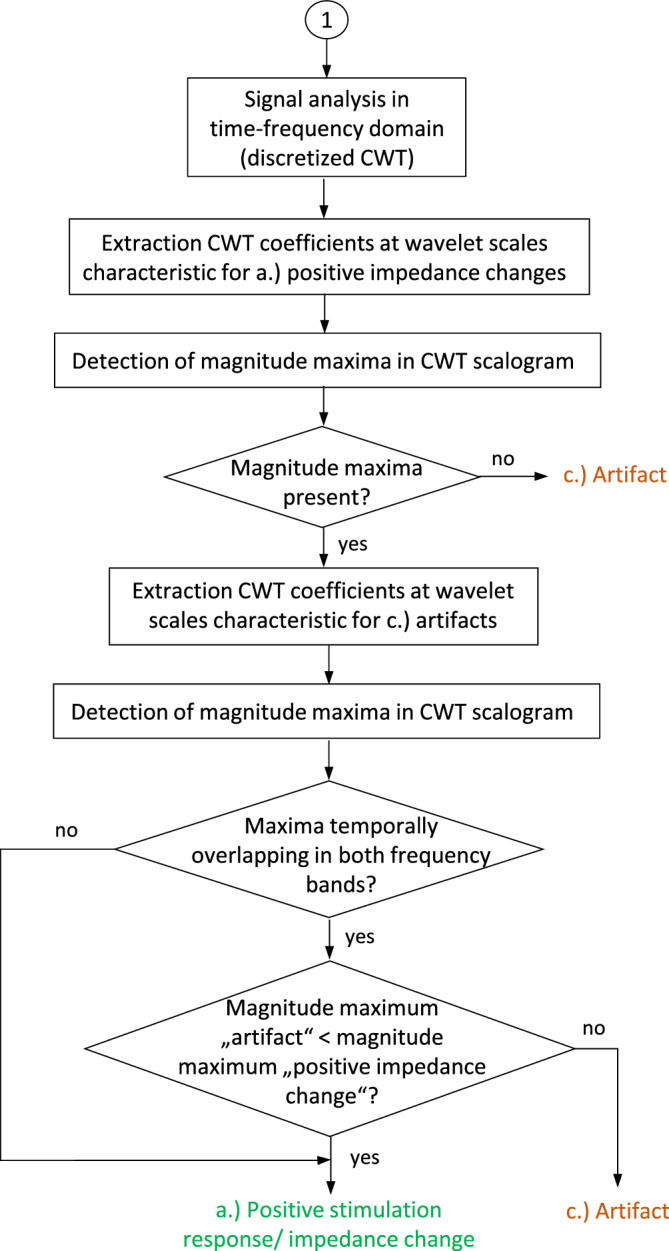
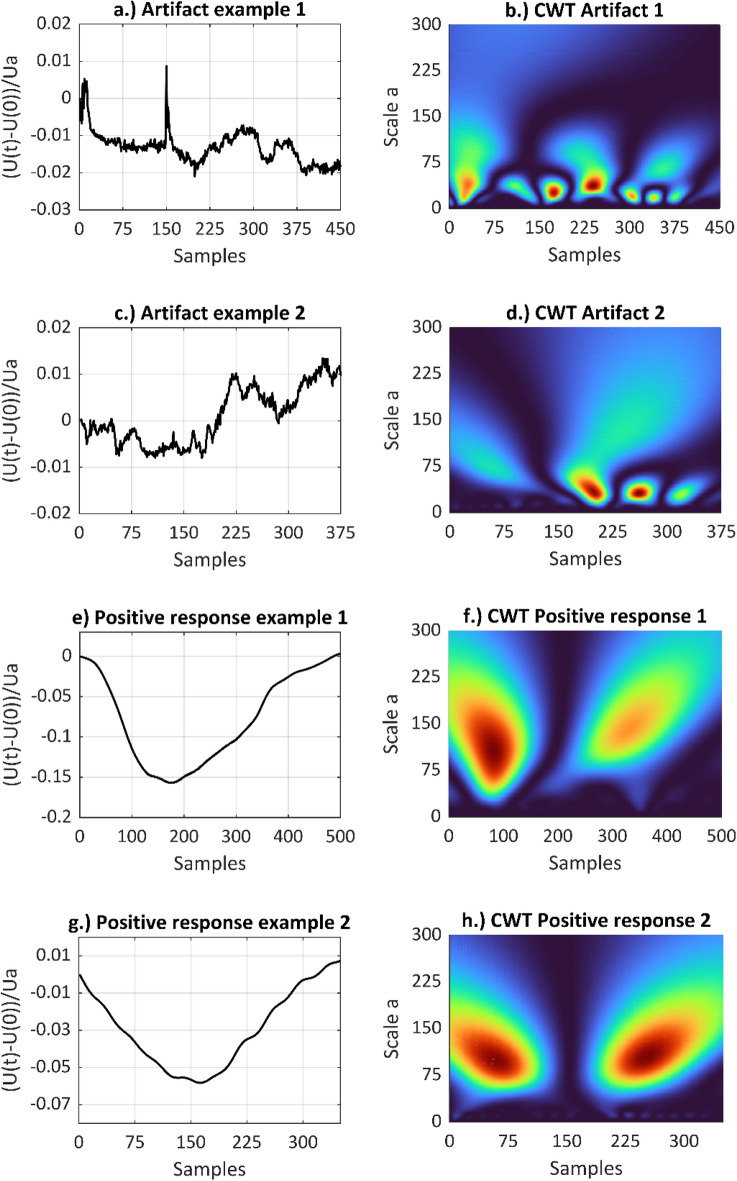
Frequent complications arising from low anterior resections include urinary and fecal incontinence, as well as sexual disorders, which are commonly associated with damage to the pelvic autonomic nerves during surgery. To assist the surgeon in preserving pelvic autonomic nerves, a novel approach for intraoperative pelvic neuromonitoring was investigated that is based on impedance measurements of the innervated organs. The objective of this work was to develop an algorithm called AMINA to classify the bioimpedance signals, with the goal of facilitating signal interpretation for the surgeon. Thirty patients included in a clinical investigation underwent nerve-preserving robotic rectal surgery using intraoperative pelvic neuromonitoring. Contraction of the urinary bladder and/or rectum, triggered by direct stimulation of the innervating nerves, resulted in a change in tissue impedance signal, allowing the nerves to be identified and preserved. Impedance signal characteristics in the time domain and the time-frequency domain were calculated and classified to develop the AMINA. Stimulation-induced positive impedance changes were statistically significantly different from negative stimulation responses by the percent amplitude of impedance change Amax in the time domain. Positive impedance changes and artifacts were distinguished by classifying wavelet scales resulting from peak detection in the continuous wavelet transform scalogram, which allowed implementation of a decision tree underlying the AMINA. The sensitivity of the software-based signal evaluation by the AMINA was 96.3%, whereas its specificity was 91.2%. This approach streamlines and automates the interpretation of impedance signals during intraoperative pelvic neuromonitoring.
© 2024. The Author(s).
Conflict of interest statement
The project was funded by the German Federal Ministry of Education and Research (see “Acknowledgements”). The authors Ramona Schuler, Maximilian Meisinger, Julia Bandura and Andreas Langer from Dr. Langer Medical GmbH hereby declare their interest in improving the prototype of a neuromonitoring device for pelvic neuromonitoring, with the aim of being able to employ this device in surgeries as part of clinical practice. All remaining authors declare no remaining conflicts of interest.
Figures


Similar articles
-
Intraoperative pelvic neuromonitoring based on bioimpedance signals: a new method analyzed on 30 patients.Langenbecks Arch Surg. 2024 Aug 3;409(1):237. doi: 10.1007/s00423-024-03403-y. Langenbecks Arch Surg. 2024. PMID: 39096391 Free PMC article.
-
Technical aspects of a new approach to intraoperative pelvic neuromonitoring during robotic rectal surgery.Sci Rep. 2023 Oct 11;13(1):17156. doi: 10.1038/s41598-023-41859-y. Sci Rep. 2023. PMID: 37821506 Free PMC article.
-
A new method of intraoperative pelvic neuromonitoring: a preclinical feasibility study in a porcine model.Sci Rep. 2022 Mar 7;12(1):3696. doi: 10.1038/s41598-022-07576-8. Sci Rep. 2022. PMID: 35256643 Free PMC article.
-
[Current research status on pelvic autonomic nerve monitoring in rectal cancer surgery].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Jan 25;25(1):82-88. doi: 10.3760/cma.j.cn441530-20210324-00130. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35067038 Review. Chinese.
-
Total mesorectal excision for rectal cancer with emphasis on pelvic autonomic nerve preservation: Expert technical tips for robotic surgery.Surg Oncol. 2015 Sep;24(3):172-80. doi: 10.1016/j.suronc.2015.06.012. Epub 2015 Jun 17. Surg Oncol. 2015. PMID: 26141555 Review.
Cited by
-
Intraoperative pelvic neuromonitoring based on bioimpedance signals: a new method analyzed on 30 patients.Langenbecks Arch Surg. 2024 Aug 3;409(1):237. doi: 10.1007/s00423-024-03403-y. Langenbecks Arch Surg. 2024. PMID: 39096391 Free PMC article.
-
[Pelvic Intraoperative Neuromonitoring - Update and Pilot Study on Telementoring].Zentralbl Chir. 2025 Aug;150(4):346-352. doi: 10.1055/a-2640-0212. Epub 2025 Aug 8. Zentralbl Chir. 2025. PMID: 40780230 Free PMC article. Review. German.
References
-
- Stelzner S, Wedel T. Anatomische Grundlagen der nervenschonenden Rektumchirurgie. Coloproctology. 2015;37:240–247. doi: 10.1007/s00053-015-0030-y. - DOI
-
- Kauff DW, Lang H, Kneist W. Risk factor analysis for newly developed urogenital dysfunction after total mesorectal excision and impact of pelvic intraoperative neuromonitoring-a prospective 2-year follow-up study. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment.Tract. 2017;21:1038–1047. doi: 10.1007/s11605-017-3409-y. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
