

Nonlinearity association between hyperuricemia and all-cause mortality in patients with chronic kidney disease
- PMID: 38182707
- PMCID: PMC10770354
- DOI: 10.1038/s41598-023-51010-6
Nonlinearity association between hyperuricemia and all-cause mortality in patients with chronic kidney disease
Abstract
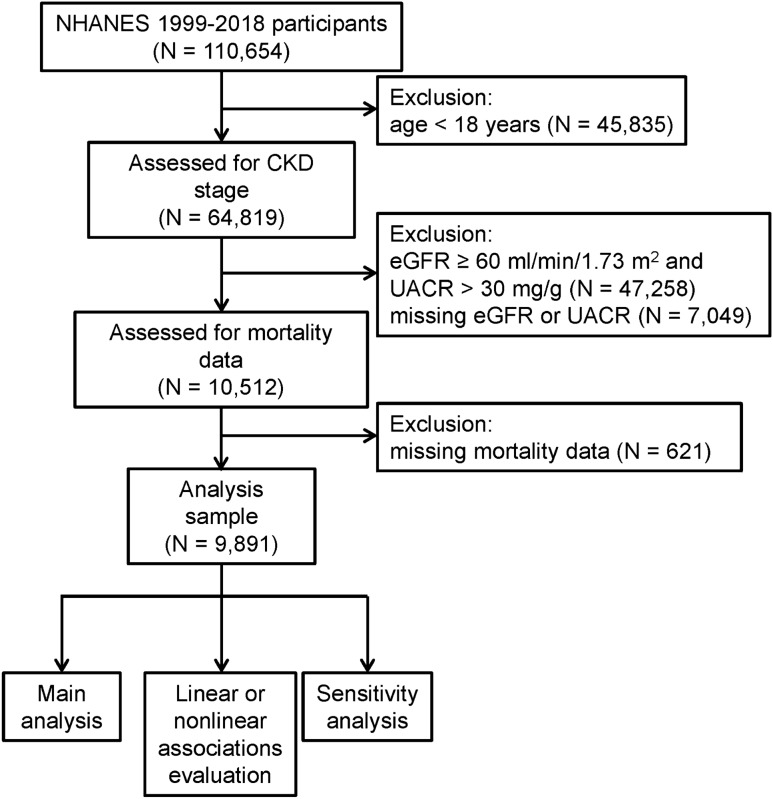
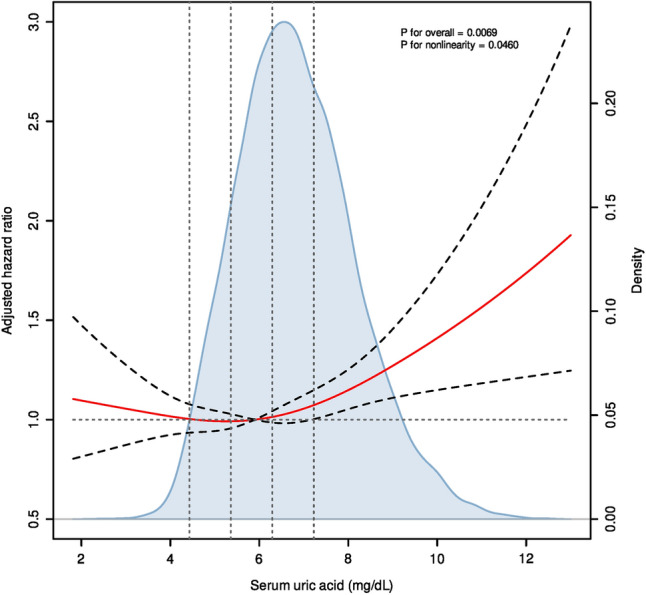
Controversy surrounds the role of serum uric acid and whether treatment intervention is favorable in retarding the progression of chronic kidney disease (CKD). The association of serum uric acid levels and CKD patient mortality risk needs to be further determined by large sample cohort studies. The National Health and Nutrition Examination Survey participants with CKD from 1998 to 2017 were enrolled in the study. Multivariable Cox regression models were used to reveal the association of serum uric acid concentrations and CKD mortality risks. A total of 9891 CKD patients were enrolled in the study, and 3698 individuals died during the follow-up. Increasing serum uric acid levels are independently relevant to higher mortality risks of CKD patients (HR per SD increase). A restricted cubic spline curve showed a nonlinear association between serum uric acid and CKD mortality risks (p for nonlinearity = 0.046). CKD patients with higher levels of serum uric acid (≥ 5.900 mg/dL) show a significant increase in mortality risks (HR = 1.102, 95% CI 1.043-1.165). Sensitivity analysis demonstrated that the results were stable and robust. High serum uric acid levels (≥ 5.900 mg/dL) may be associated with increased mortality risks in CKD patients.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
