

Maternal and neonatal outcomes according to the timing of diagnosis of hyperglycaemia in pregnancy: a nationwide cross-sectional study of 695,912 deliveries in France in 2018
- PMID: 38182910
- PMCID: PMC10844424
- DOI: 10.1007/s00125-023-06066-4
Maternal and neonatal outcomes according to the timing of diagnosis of hyperglycaemia in pregnancy: a nationwide cross-sectional study of 695,912 deliveries in France in 2018
Abstract
Aims/hypothesis: We aimed to assess maternal-fetal outcomes according to various subtypes of hyperglycaemia in pregnancy.
Methods: We used data from the French National Health Data System (Système National des Données de Santé), which links individual data from the hospital discharge database and the French National Health Insurance information system. We included all deliveries after 22 gestational weeks (GW) in women without pre-existing diabetes recorded in 2018. Women with hyperglycaemia were classified as having overt diabetes in pregnancy or gestational diabetes mellitus (GDM), then categorised into three subgroups according to their gestational age at the time of GDM diagnosis: before 22 GW (GDM<22); between 22 and 30 GW (GDM22-30); and after 30 GW (GDM>30). Adjusted prevalence ratios (95% CI) for the outcomes were estimated after adjusting for maternal age, gestational age and socioeconomic status. Due to the multiple tests, we considered an association to be statistically significant according to the Holm-Bonferroni procedure. To take into account the potential immortal time bias, we performed analyses on deliveries at ≥31 GW and deliveries at ≥37 GW.
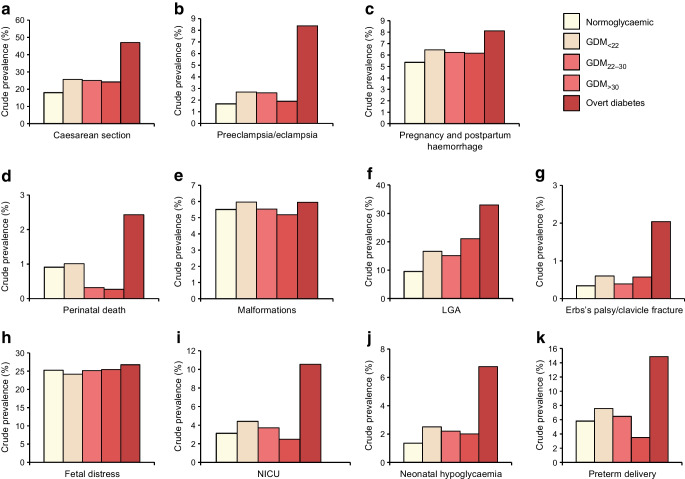
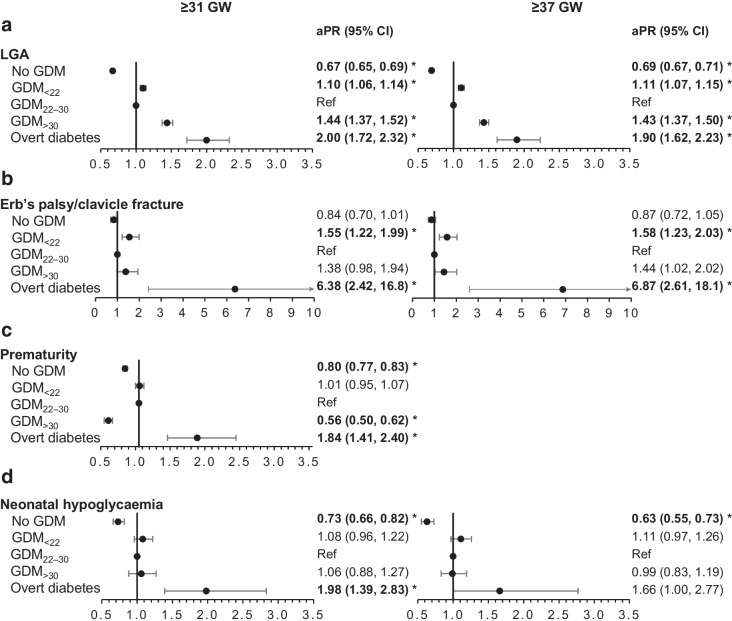
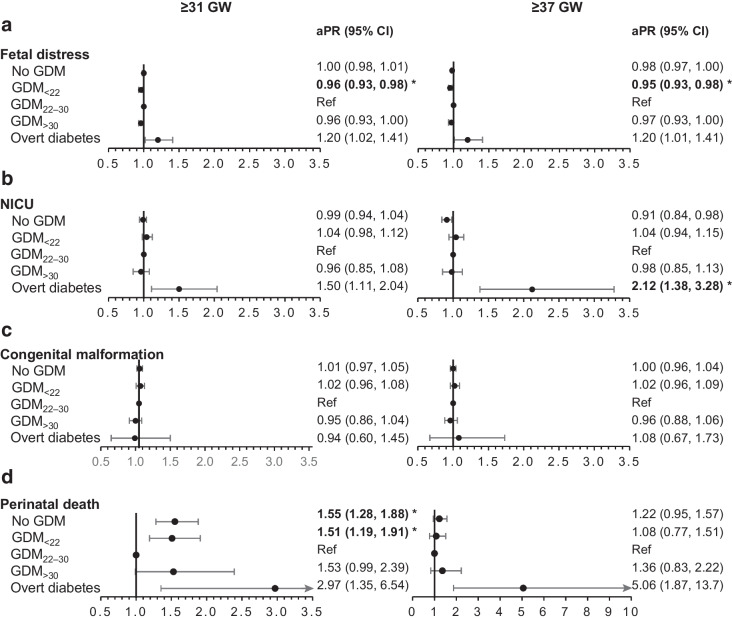
Results: The study population of 695,912 women who gave birth in 2018 included 84,705 women (12.2%) with hyperglycaemia in pregnancy: overt diabetes in pregnancy, 0.4%; GDM<22, 36.8%; GDM22-30, 52.4%; and GDM>30, 10.4%. The following outcomes were statistically significant after Holm-Bonferroni adjustment for deliveries at ≥31 GW using GDM22-30 as the reference. Caesarean sections (1.54 [1.39, 1.72]), large-for-gestational-age (LGA) infants (2.00 [1.72, 2.32]), Erb's palsy or clavicle fracture (6.38 [2.42, 16.8]), preterm birth (1.84 [1.41, 2.40]) and neonatal hypoglycaemia (1.98 [1.39, 2.83]) were more frequent in women with overt diabetes. Similarly, LGA infants (1.10 [1.06, 1.14]) and Erb's palsy or clavicle fracture (1.55 [1.22, 1.99]) were more frequent in GDM<22. LGA infants (1.44 [1.37, 1.52]) were more frequent in GDM>30. Finally, women without hyperglycaemia in pregnancy were less likely to have preeclampsia or eclampsia (0.74 [0.69, 0.79]), Caesarean section (0.80 [0.79, 0.82]), pregnancy and postpartum haemorrhage (0.93 [0.89, 0.96]), LGA neonate (0.67 [0.65, 0.69]), premature neonate (0.80 [0.77, 0.83]) and neonate with neonatal hypoglycaemia (0.73 [0.66, 0.82]). Overall, the results were similar for deliveries at ≥37 GW. Although the estimation of the adjusted prevalence ratio of perinatal death was five times higher (5.06 [1.87, 13.7]) for women with overt diabetes, this result was non-significant after Holm-Bonferroni adjustment.
Conclusions/interpretation: Compared with GDM22-30, overt diabetes, GDM<22 and, to a lesser extent, GDM>30 were associated with poorer maternal-fetal outcomes.
Keywords: Caesarean section; Diabetes; Gestational diabetes mellitus; Macrosomia; Overt diabetes in pregnancy; Perinatal death; Preeclampsia; Pregnancy; Prematurity.
© 2024. The Author(s).
Figures

Similar articles
-
Gestational diabetes and adverse perinatal outcomes from 716,152 births in France in 2012.Diabetologia. 2017 Apr;60(4):636-644. doi: 10.1007/s00125-017-4206-6. Epub 2017 Feb 15. Diabetologia. 2017. PMID: 28197657 Free PMC article.
-
Weight gain after diagnosis of gestational diabetes mellitus and its association with adverse pregnancy outcomes: a cohort study.BMC Pregnancy Childbirth. 2021 Mar 17;21(1):216. doi: 10.1186/s12884-021-03690-z. BMC Pregnancy Childbirth. 2021. PMID: 33731035 Free PMC article.
-
Maternal and neonatal outcomes and time trends of gestational diabetes mellitus in Sweden from 1991 to 2003.Diabet Med. 2010 Apr;27(4):436-41. doi: 10.1111/j.1464-5491.2010.02978.x. Diabet Med. 2010. PMID: 20536516
-
Screening and diagnosing gestational diabetes mellitus.Evid Rep Technol Assess (Full Rep). 2012 Oct;(210):1-327. Evid Rep Technol Assess (Full Rep). 2012. PMID: 24423035 Free PMC article. Review.
-
Perinatal Outcomes and Related Risk Factors of Single vs Twin Pregnancy Complicated by Gestational Diabetes Mellitus: Meta-Analysis.Comput Math Methods Med. 2022 Jul 4;2022:3557890. doi: 10.1155/2022/3557890. eCollection 2022. Comput Math Methods Med. 2022. PMID: 35832130 Free PMC article. Review.
Cited by
-
Antagonistic effects of smoking and maternal glycemia on fetal growth: a retrospective study among 13,958 pregnant French women.Front Endocrinol (Lausanne). 2025 Mar 14;16:1527358. doi: 10.3389/fendo.2025.1527358. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40162319 Free PMC article.
-
Unveiling Gestational Diabetes: An Overview of Pathophysiology and Management.Int J Mol Sci. 2025 Mar 5;26(5):2320. doi: 10.3390/ijms26052320. Int J Mol Sci. 2025. PMID: 40076938 Free PMC article. Review.
-
A new classification method for gestational diabetes mellitus: a study on the relationship between abnormal blood glucose values at different time points in oral glucose tolerance test and adverse maternal and neonatal outcomes in pregnant women with gestational diabetes mellitus.AJOG Glob Rep. 2024 Aug 15;4(4):100390. doi: 10.1016/j.xagr.2024.100390. eCollection 2024 Nov. AJOG Glob Rep. 2024. PMID: 39309607 Free PMC article.
-
Comparative analysis of perinatal outcomes in pregnant women with pregestational diabetes mellitus based on diagnostic timing.Sci Rep. 2025 Mar 20;15(1):9613. doi: 10.1038/s41598-025-93449-9. Sci Rep. 2025. PMID: 40113921 Free PMC article.
-
Effectiveness of a risk perception-based nursing model for high-risk pregnant women with gestational diabetes: A retrospective cohort study.Medicine (Baltimore). 2025 Jul 25;104(30):e43311. doi: 10.1097/MD.0000000000043311. Medicine (Baltimore). 2025. PMID: 40725938 Free PMC article.
References
-
- Sacks DA, Hadden DR, Maresh M, et al. Frequency of gestational diabetes mellitus at collaborating centers based on IADPSG consensus panel-recommended criteria: the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study. Diabetes Care. 2012;35(3):526–528. doi: 10.2337/dc11-1641. - DOI - PMC - PubMed
-
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. Metzger BE, Gabbe SG, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676–682. doi: 10.2337/dc09-1848. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
