

Adult-type anomalous origin of the left coronary artery from the pulmonary artery and right coronary-right atrial fistula: a case report
- PMID: 38183012
- PMCID: PMC10768160
- DOI: 10.1186/s12872-023-03686-x
Adult-type anomalous origin of the left coronary artery from the pulmonary artery and right coronary-right atrial fistula: a case report
Abstract
Background: Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) is a rare congenital cardiac anomaly, mortality rates in infancy reach approximately 90%, with only a small number of patients surviving into adulthood, therefore, most of the literature reports mainly focus on infantile type.
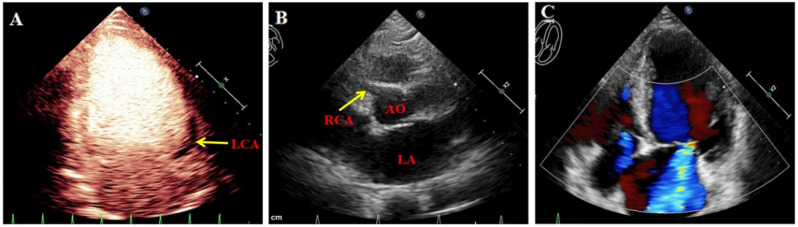
Case presentation: A 55-year-old female was admitted due to persistent repeated chest pain experienced and had worsened for unknown reasons. Color doppler echocardiography, coronary computed tomographic angiography, and coronary angiography confirmed the diagnosis of ALCAPA and concurrent right coronary artery-right atrial fistula. The symptoms of chest pain exhibited notable improvement subsequent to corrective surgery for the anomalous origin of the coronary artery.
Conclusions: This report shows an unique case of ALCAPA in an adult patient, characterizing the condition's combination with a right coronary-right atrial fistula, and it is prone to misdiagnosis and misdiagnosis. We aim to provide valuable insights for clinical diagnosis and treatment of ALCAPA.
Keywords: ALCAPA; Congenital heart disease; Coronary artery fistula; Surgical intervention.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Two congenital coronary abnormalities affecting heart function: anomalous origin of the left coronary artery from the pulmonary artery and congenital left main coronary artery atresia.Chin Med J (Engl). 2014;127(21):3724-31. Chin Med J (Engl). 2014. PMID: 25382327
-
[Analysis on missed diagnosis or misdiagnosis of anomalous origin of left coronary artery from pulmonary artery by echocardiography from one single medical center].Zhonghua Xin Xue Guan Bing Za Zhi. 2023 May 24;51(5):481-489. doi: 10.3760/cma.j.cn112148-20220712-00541. Zhonghua Xin Xue Guan Bing Za Zhi. 2023. PMID: 37198119 Chinese.
-
Adult-type ALCAPA syndrome: A rare coronary artery anomaly.Echocardiography. 2018 Jul;35(7):1056-1059. doi: 10.1111/echo.14013. Epub 2018 May 11. Echocardiography. 2018. PMID: 29749648
-
Acute myocardial infarction in the elderly with anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA): A case report and literature review.Medicine (Baltimore). 2022 Dec 2;101(48):e32219. doi: 10.1097/MD.0000000000032219. Medicine (Baltimore). 2022. PMID: 36482632 Free PMC article. Review.
-
The management of the older adult patient with anomalous left coronary artery from the pulmonary artery syndrome: a presentation of two cases and review of the literature.Congenit Heart Dis. 2014 Nov-Dec;9(6):E185-94. doi: 10.1111/chd.12125. Epub 2013 Aug 18. Congenit Heart Dis. 2014. PMID: 23953779 Review.
Cited by
-
Coronary ostial stenosis in an infant with nonischemic anomalous left coronary artery from the pulmonary artery.Ann Pediatr Cardiol. 2025 Jan-Feb;18(1):79-80. doi: 10.4103/apc.apc_145_25. Epub 2025 Jul 14. Ann Pediatr Cardiol. 2025. PMID: 40814326 Free PMC article.
-
An adult case of Bland-White-Garland syndrome with Vieussens' arterial ring.Eur Heart J Case Rep. 2024 Sep 2;8(9):ytae468. doi: 10.1093/ehjcr/ytae468. eCollection 2024 Sep. Eur Heart J Case Rep. 2024. PMID: 39286731 Free PMC article. No abstract available.
References
-
- Neumann A, Sarikouch S, Bobylev D, Meschenmoser L, Breymann T, Westhoff-Bleck M, et al. Long-term results after repair of anomalous origin of left coronary artery from the pulmonary artery: Takeuchi repair versus coronary transfer. Eur J Cardiothorac Surg. 2017;51(2):308–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
