

Comparison of clinical outcomes between sequestered cervical disk herniation and non-sequestered cervical disk herniation after anterior cervical decompression and fusion: a cohort study
- PMID: 38183107
- PMCID: PMC10771008
- DOI: 10.1186/s13018-023-04515-9
Comparison of clinical outcomes between sequestered cervical disk herniation and non-sequestered cervical disk herniation after anterior cervical decompression and fusion: a cohort study
Abstract
Background: The advantages of anterior cervical decompression and fusion (ACDF) were well published, while research on postoperative results in different subtypes of cervical disk herniation (CDH) still remains blank. This study aimed to explore the surgical outcome between sequestration and other types in CDH.
Methods: This retrospective cohort study enrolled 108 patients treated with ACDF in our hospital. The participants were divided into two groups according to the existence of a sequestered disk. The Visual analog scale score, the Japanese Orthopedics Association (JOA) score and the Neck disability index score were used to evaluate postoperative outcome.
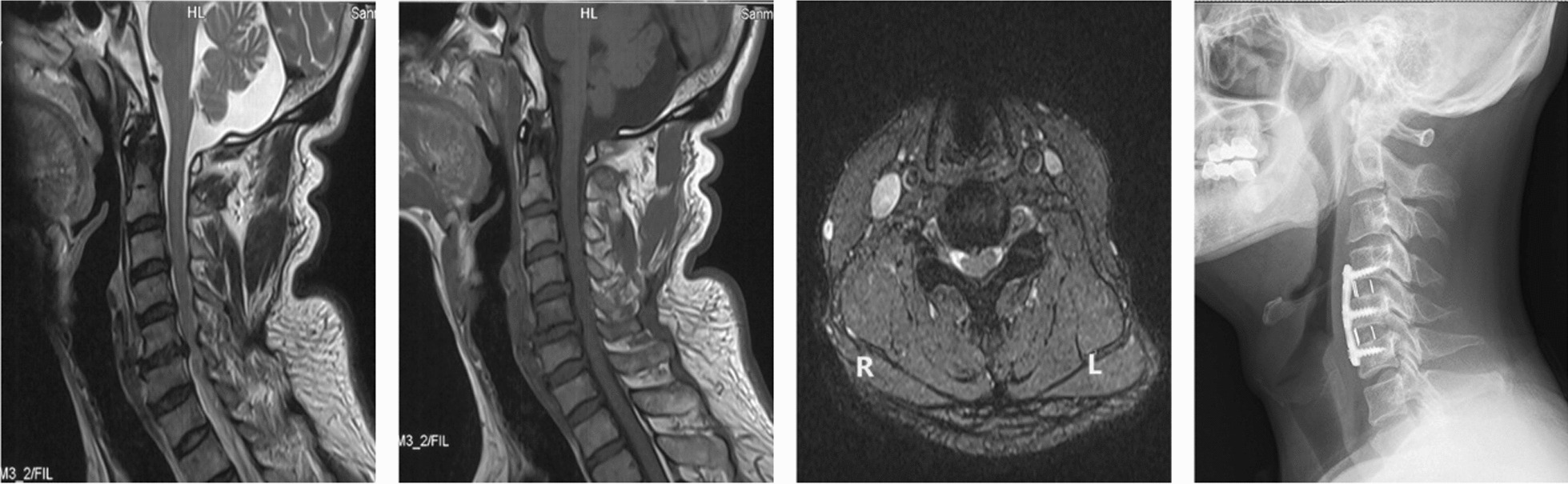
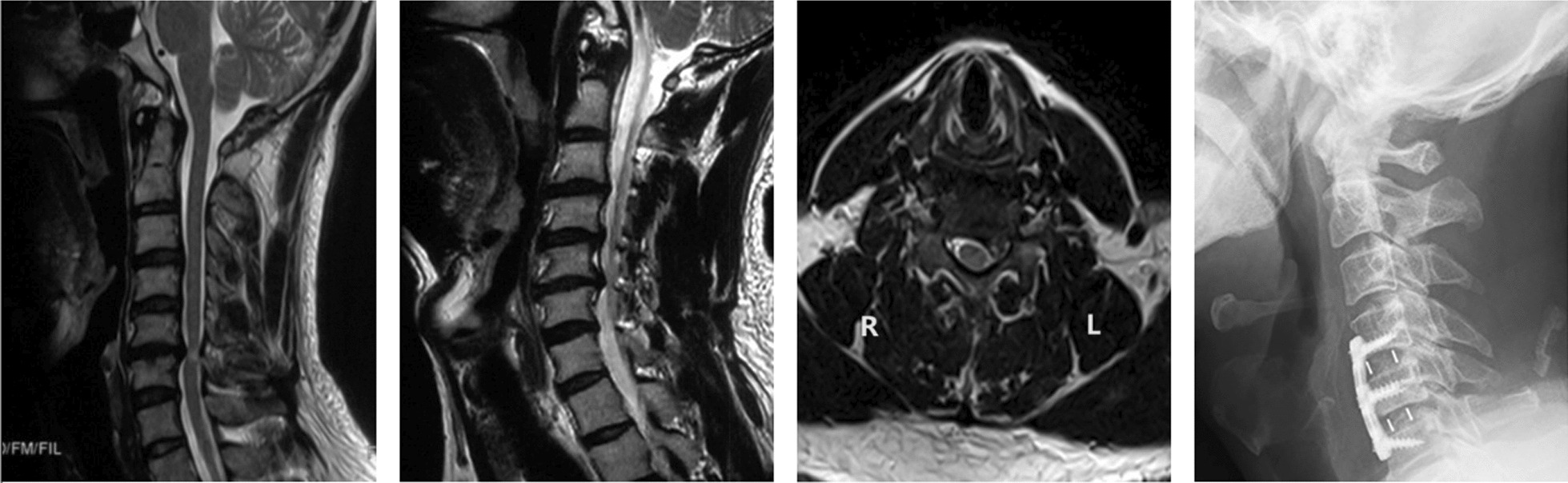
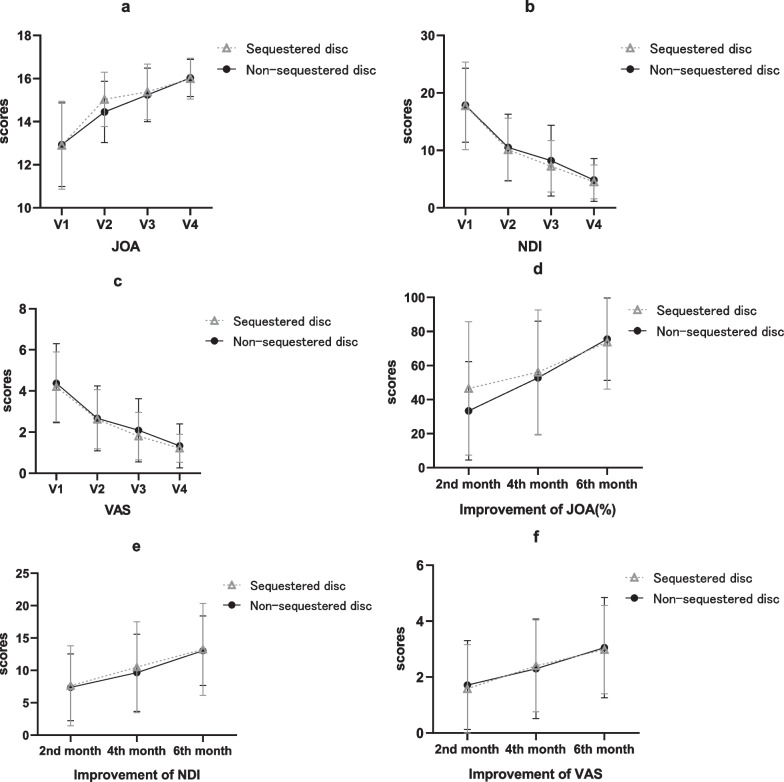
Results: Significant improvements were observed in both groups at every viewpoint (P < 0.001). The mean JOA was 15.04 ± 1.26 in the sequestered disk group and 14.45 ± 1.43 in the non-sequestered disk group two months after the operation (P = 0.026 < 0.05). The improvement in JOA at two months after ACDF showed a significant difference: 46.58% ± 39.17% in the sequestered disk group and 33.39% ± 28.82% in the non-sequestered disk group (P = 0.047 < 0.05). Thirty-two patients in the sequestered disk group (64%) and 19 patients in the non-sequestered disk group (32.76%) presented with high signal intensity of the spinal cord on preoperative cervical T2-weighted MRI (P < 0.001).
Conclusions: Patients with sequestered cervical disks seemed to have a higher degree of symptom improvement two months after ACDF. CDH with a sequestered disk appears to be more likely to cause high signal intensity changes in the compressed cervical spine on T2-weighted MRI. We prefer early positive surgery in patients with sequestered cervical disks from the clinical point of view.
Keywords: Anterior cervical decompression and fusion; Cervical spine; Cord signal change; Outcomes; Sequestered disk.
© 2024. The Author(s).
Conflict of interest statement
All authors have read and approved the content, certify that this manuscript is a unique submission and is not being considered for publication, in part or in full, with any other source in any medium. There are no ethical/legal conflicts involved in the article.
Figures


Similar articles
-
Anterior cervical discectomy and fusion for the treatment of giant cervical disc herniation.J Orthop Surg Res. 2023 Sep 13;18(1):683. doi: 10.1186/s13018-023-04036-5. J Orthop Surg Res. 2023. PMID: 37705025 Free PMC article.
-
[Analysis of clinical effects of cervical artificial disc replacement or anterior cervical decompression and fusion for the treatment of single cervical disc herniation].Zhongguo Gu Shang. 2015 Jan;28(1):21-5. Zhongguo Gu Shang. 2015. PMID: 25823126 Chinese.
-
Anterior transcorporeal approach of percutaneous endoscopic cervical discectomy for disc herniation at the C4-C5 levels: a technical note.Spine J. 2016 May;16(5):659-66. doi: 10.1016/j.spinee.2016.01.187. Epub 2016 Feb 2. Spine J. 2016. PMID: 26850173
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Mid-Term to Long-Term Outcomes After Total Cervical Disk Arthroplasty Compared With Anterior Diskectomy and Fusion: A Systematic Review and Meta-analysis of Randomized Controlled Trials.Clin Spine Surg. 2020 Jun;33(5):192-200. doi: 10.1097/BSD.0000000000000929. Clin Spine Surg. 2020. PMID: 32271175
References
-
- Fardon DF, Williams AL, Dohring EJ, Murtagh FR, Gabriel Rothman SL, Sze GK. Lumbar disc nomenclature: version 2.0 recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology, and the American Society of Neuroradiology. Spine (Phila Pa 1976) 2014;39(24):E1448–1465. doi: 10.1097/BRS.0b013e3182a8866d. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
