

A predictive nomogram for surgical site infection in patients who received clean orthopedic surgery: a retrospective study
- PMID: 38183110
- PMCID: PMC10770936
- DOI: 10.1186/s13018-023-04473-2
A predictive nomogram for surgical site infection in patients who received clean orthopedic surgery: a retrospective study
Abstract
Background: Surgical site infection (SSI) is a common and serious complication of elective clean orthopedic surgery that can lead to severe adverse outcomes. However, the prognostic efficacy of the current staging systems remains uncertain for patients undergoing elective aseptic orthopedic procedures. This study aimed to identify high-risk factors independently associated with SSI and develop a nomogram prediction model to accurately predict the occurrence of SSI.
Methods: A total of 20,960 patients underwent elective clean orthopedic surgery in our hospital between January 2020 and December 2021, of whom 39 developed SSI; we selected all 39 patients with a postoperative diagnosis of SSI and 305 patients who did not develop postoperative SSI for the final analysis. The patients were randomly divided into training and validation cohorts in a 7:3 ratio. Univariate and multivariate logistic regression analyses were conducted in the training cohort to screen for independent risk factors of SSI, and a nomogram prediction model was developed. The predictive performance of the nomogram was compared with that of the National Nosocomial Infections Surveillance (NNIS) system. Decision curve analysis (DCA) was used to assess the clinical decision-making value of the nomogram.
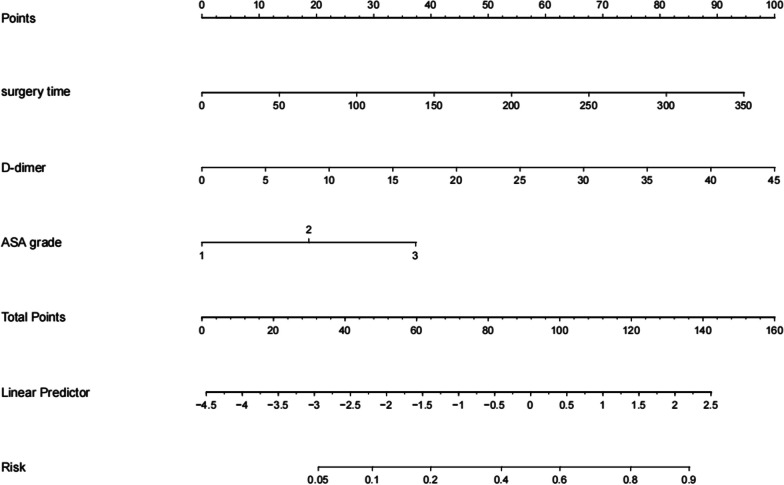
Results: The SSI incidence was 0.186%. Univariate and multivariate logistic regression analysis identified the American Society of Anesthesiology (ASA) class (odds ratio [OR] 1.564 [95% confidence interval (CI) 1.029-5.99, P = 0.046]), operative time (OR 1.003 [95% CI 1.006-1.019, P < 0.001]), and D-dimer level (OR 1.055 [95% CI 1.022-1.29, P = 0.046]) as risk factors for postoperative SSI. We constructed a nomogram prediction model based on these independent risk factors. In the training and validation cohorts, our predictive model had concordance indices (C-indices) of 0.777 (95% CI 0.672-0.882) and 0.732 (95% CI 0.603-0.861), respectively, both of which were superior to the C-indices of the NNIS system (0.668 and 0.543, respectively). Calibration curves and DCA confirmed that our nomogram model had good consistency and clinical predictive value, respectively.
Conclusions: Operative time, ASA class, and D-dimer levels are important clinical predictive indicators of postoperative SSI in patients undergoing elective clean orthopedic surgery. The nomogram predictive model based on the three clinical features demonstrated strong predictive performance, calibration capabilities, and clinical decision-making abilities for SSI.
Keywords: Elective clean orthopedic surgery; Nomogram; Prediction model; Surgical site infection.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Development and validation of a nomogram to predict the risk of surgical site infection within 1 month after transforaminal lumbar interbody fusion.J Orthop Surg Res. 2023 Feb 14;18(1):105. doi: 10.1186/s13018-023-03550-w. J Orthop Surg Res. 2023. PMID: 36788621 Free PMC article.
-
A nomogram to predict postoperative surgical site infection of adult patients who received orthopaedic surgery: a retrospective study.Sci Rep. 2023 May 19;13(1):8129. doi: 10.1038/s41598-023-34926-x. Sci Rep. 2023. PMID: 37208366 Free PMC article.
-
Construction and validation of nomogram to predict surgical site infection after hysterectomy: a retrospective study.Sci Rep. 2024 Sep 4;14(1):20538. doi: 10.1038/s41598-024-71592-z. Sci Rep. 2024. PMID: 39232052 Free PMC article.
-
Development and validation of a preoperative systemic inflammation-based nomogram for predicting surgical site infection in patients with colorectal cancer.Int J Colorectal Dis. 2024 Dec 21;39(1):208. doi: 10.1007/s00384-024-04772-y. Int J Colorectal Dis. 2024. PMID: 39707016 Free PMC article. Review.
-
Surgical site infection in elective clean and clean-contaminated surgeries in developing countries.Int J Infect Dis. 2019 Mar;80:34-45. doi: 10.1016/j.ijid.2018.12.013. Epub 2019 Jan 9. Int J Infect Dis. 2019. PMID: 30639405
Cited by
-
Development and validation of a nomogram to predict the risk of adjacent segment disease after transforaminal lumbar interbody fusion in patients with lumbar degenerative diseases.J Orthop Surg Res. 2024 Oct 22;19(1):680. doi: 10.1186/s13018-024-05170-4. J Orthop Surg Res. 2024. PMID: 39438978 Free PMC article.
-
Construction and validation of a predictive in-hospital mortality nomogram in patients with staphylococcus aureus bloodstream infection.Sci Rep. 2025 Aug 13;15(1):29658. doi: 10.1038/s41598-025-15826-8. Sci Rep. 2025. PMID: 40804334 Free PMC article.
-
Development and validation of a predictive nomogram for surgical site infection among general surgery patients in Amhara region Ethiopia.Sci Rep. 2025 Mar 25;15(1):10322. doi: 10.1038/s41598-025-85939-7. Sci Rep. 2025. PMID: 40133411 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
