

Predictive Factors for Residual Low Back Pain Following Percutaneous Endoscopic Lumbar Discectomy in Patients with Lumbar Disc Herniation
- PMID: 38183217
- PMCID: PMC10777582
- DOI: 10.12659/MSM.942231
Predictive Factors for Residual Low Back Pain Following Percutaneous Endoscopic Lumbar Discectomy in Patients with Lumbar Disc Herniation
Abstract
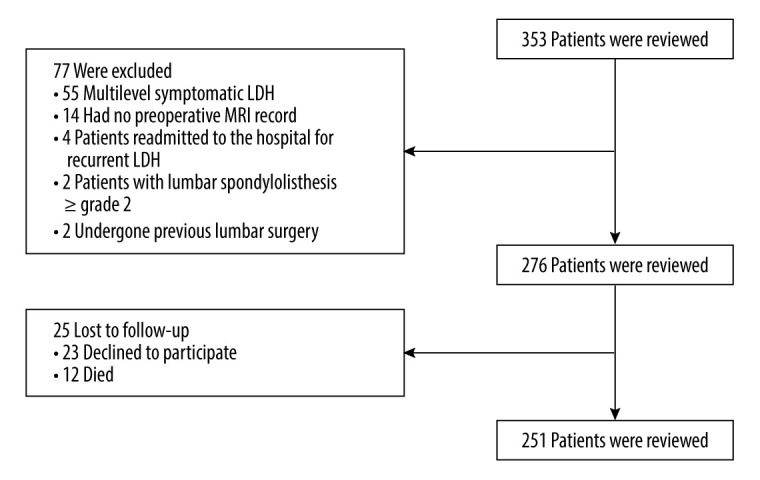
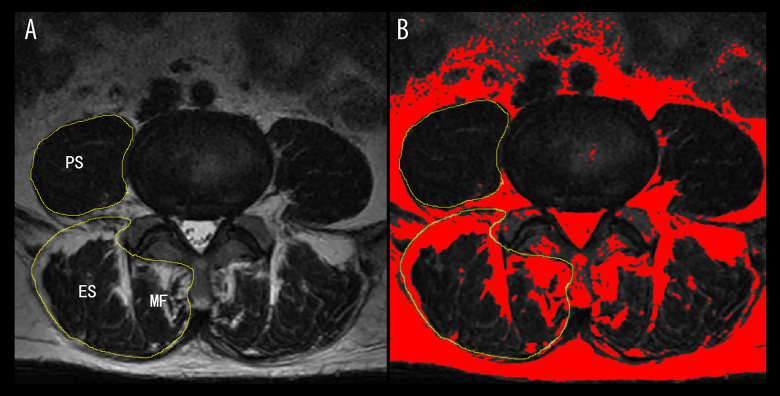
BACKGROUND Percutaneous endoscopic lumbar discectomy (PELD) is a mature and popular surgery for treatment of lumbar disc herniation (LDH). The main objective of our study was to identify risk factors for residual low back pain after PELD and to improve postoperative management. MATERIAL AND METHODS We retrospectively analyzed the clinical and imaging data of 251 patients who underwent PELD for LDH. We defined residual LBP as visual analog scale (VAS) score for LBP ≥3 at 2 years postoperatively, and severe LBP was defined as VAS for LBP ≥7.5. The clinical and imaging data were analyzed by comparing patients with VAS scores ≥3 and <3, and univariate analysis and multivariable logistic regression analysis were applied to predict the risk factors for residual LBP. RESULTS There were 56 (22.3%) patients with LBP VAS ≥3 at 2 years postoperatively. Multivariable logistic regression analysis demonstrated that severe baseline VAS for LBP (P<0.001), MCs type I (P=0.006), and severe fatty infiltration of the paravertebral muscles (P<0.001) were independent risk factors for residual LBP after PELD. CONCLUSIONS In patients with LDH, MCs type I, severe baseline LBP, and fatty infiltration of the paravertebral muscles were predictive factors for residual LBP after PELD. Our study suggests that spine surgeons should pay more attention to these imaging parameters, which may be a helpful indicator for the choice of surgical modality.
Conflict of interest statement
Figures
Similar articles
-
Efficacy of percutaneous endoscopic lumbar discectomy (PELD) combined with sinuvertebral nerve ablation versus PELD for low back pain in lumbar disc herniation.J Orthop Surg Res. 2024 Nov 19;19(1):769. doi: 10.1186/s13018-024-05269-8. J Orthop Surg Res. 2024. PMID: 39563398 Free PMC article.
-
Varied Low Back Pain Induced by Different Spinal Tissues in Percutaneous Endoscopic Lumbar Discectomy: A Retrospective Study.Pain Physician. 2022 Mar;25(2):E331-E339. Pain Physician. 2022. PMID: 35322988
-
Comparison of percutaneous endoscopic transforaminal discectomy, microendoscopic discectomy, and microdiscectomy for symptomatic lumbar disc herniation: minimum 2-year follow-up results.J Neurosurg Spine. 2018 Mar;28(3):317-325. doi: 10.3171/2017.6.SPINE172. Epub 2018 Jan 5. J Neurosurg Spine. 2018. PMID: 29303471
-
Comparison of percutaneous endoscopic lumbar discectomy versus microendoscopic discectomy for the treatment of lumbar disc herniation: a meta-analysis.Int Orthop. 2019 Apr;43(4):923-937. doi: 10.1007/s00264-018-4253-8. Epub 2018 Dec 13. Int Orthop. 2019. PMID: 30547214
-
Percutaneous Endoscopic Lumbar Discectomy Versus Posterior Open Lumbar Microdiscectomy for the Treatment of Symptomatic Lumbar Disc Herniation: A Systemic Review and Meta-Analysis.World Neurosurg. 2018 Dec;120:352-362. doi: 10.1016/j.wneu.2018.08.236. Epub 2018 Sep 8. World Neurosurg. 2018. PMID: 30205219
Cited by
-
Effects of dynamic stabilization and fusion on postoperative paraspinal muscle degeneration and lumbar function recovery.J Orthop Surg Res. 2025 May 30;20(1):552. doi: 10.1186/s13018-025-05837-6. J Orthop Surg Res. 2025. PMID: 40448178 Free PMC article.
References
-
- Kambin P, Sampson S. Posterolateral percutaneous suction-excision of herniated lumbar intervertebral discs. Report of interim results. Clin Orthop Relat Res. 1986;(207):37–43. - PubMed
-
- Cong L, Zhu Y, Tu G. A meta-analysis of endoscopic discectomy versus open discectomy for symptomatic lumbar disk herniation. Eur Spine J. 2016;25(1):134–43. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
