

Birth asphyxia and its association with grand multiparity and referral among hospital births: A prospective cross-sectional study in Benin, Malawi, Tanzania and Uganda
- PMID: 38183308
- PMCID: PMC10867390
- DOI: 10.1111/aogs.14754
Birth asphyxia and its association with grand multiparity and referral among hospital births: A prospective cross-sectional study in Benin, Malawi, Tanzania and Uganda
Abstract
Introduction: Birth asphyxia is a leading cause of neonatal mortality in sub-Saharan Africa. The relationship to grand multiparity (GM), a controversial pregnancy risk factor, remains largely unexplored, especially in the context of large multinational studies. We investigated birth asphyxia and its association with GM and referral in Benin, Malawi, Tanzania and Uganda.
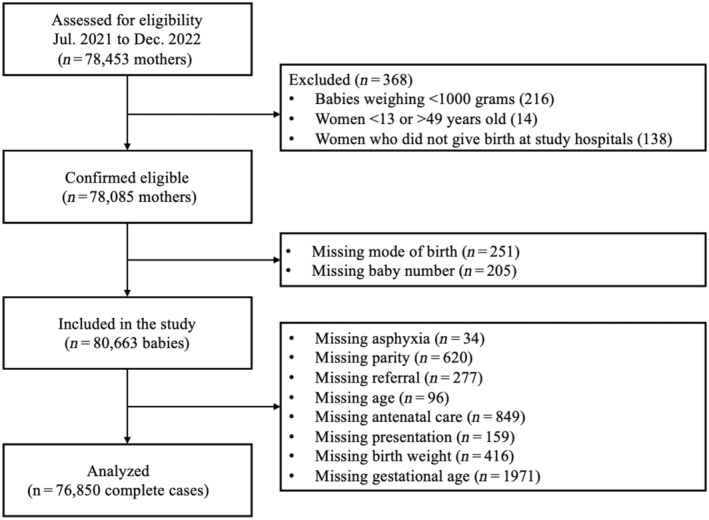
Material and methods: This was a prospective cross-sectional study. Data were collected using a perinatal e-Registry in 16 hospitals (four per country). The study population consisted of 80 663 babies (>1000 g, >28 weeks' gestational age) delivered between July 2021 and December 2022. The primary outcome was birth asphyxia, defined by 5-minute appearance, pulse, grimace, activity and respiration score <7. A multilevel and stratified multivariate logistic regression was performed with GM (parity ≥5) as exposure, and birth asphyxia as outcome. An interaction between referral (none, prepartum, intrapartum) and GM was also evaluated as a secondary outcome. All models were adjusted for confounders.
Clinical trial: Pan African Clinical Trial Registry 202006793783148.
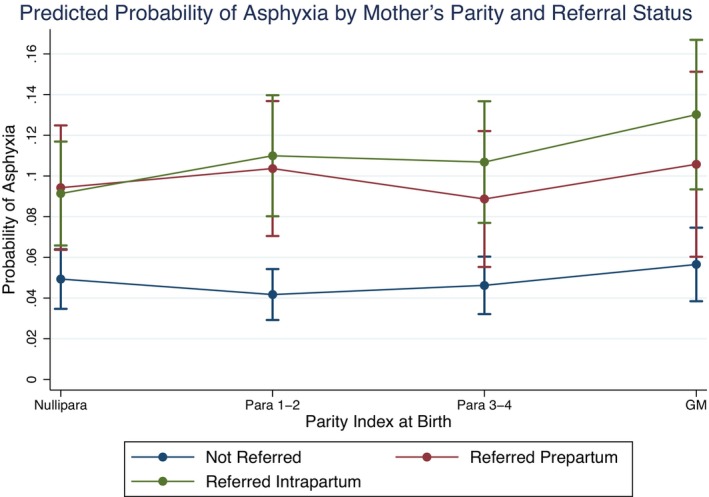
Results: Birth asphyxia was present in 7.0% (n = 5612) of babies. More babies with birth asphyxia were born to grand multiparous women (11.9%) than to other parity groups (≤7.6%). Among the 76 850 cases included in the analysis, grand multiparous women had a 1.34 times higher odds of birth asphyxia (95% confidence interval [CI] 1.17-1.54) vs para one to two. Grand multiparous women referred intrapartum had the highest probability of asphyxiation (13.02%, 95% CI 9.34-16.69). GM increased odds of birth asphyxia in Benin (odds ratio [OR] 1.37, 95% CI 1.13-1.68) and Uganda (OR 1.29, 95% CI 1.02-1.64), but was non-significant in Tanzania (OR 1.44, 95% CI 0.81-2.56) and Malawi (OR 0.98, 95% CI 0.67-1.44).
Conclusions: There is some evidence of an increased risk of birth asphyxia for grand multiparous women having babies at hospitals, especially following intrapartum referral. Antenatal counseling should recognize grand multiparity as higher risk and advise appropriate childbirth facilities. Findings in Malawi suggest an advantage of health systems configuration requiring further exploration.
Keywords: high-risk; low-income country; obstetrics; pregnancy; pregnancy birth.
© 2024 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
None declared.
Figures


References
-
- UN Inter‐Agency Group for Child Mortality Estimation . Child Mortality and Stillbirth Estimates [Internet]. ChildMortality.org. https://childmortality.org/
-
- World Health Organization . Guidelines on Basic Newborn Resuscitation [Internet]. 2012. Geneva: World Health Organization. Accessed May 30, 2023. https://apps.who.int/iris/handle/10665/75157
-
- Casey BM, McIntire DD, Leveno KJ. The continuing value of the Apgar score for the assessment of newborn infants. N Engl J Med. 2001;344:467‐471. - PubMed
-
- Igboanugo S, Chen A, Mielke JG. Maternal risk factors for birth asphyxia in low‐resource communities. A systematic review of the literature. J Obstet Gynaecol. 2020;40:1039‐1055. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
