

Association of random and observed urine drug screening with long-term retention in opioid treatment programs
- PMID: 38183832
- PMCID: PMC10956422
- DOI: 10.1016/j.drugalcdep.2023.111067
Association of random and observed urine drug screening with long-term retention in opioid treatment programs
Abstract
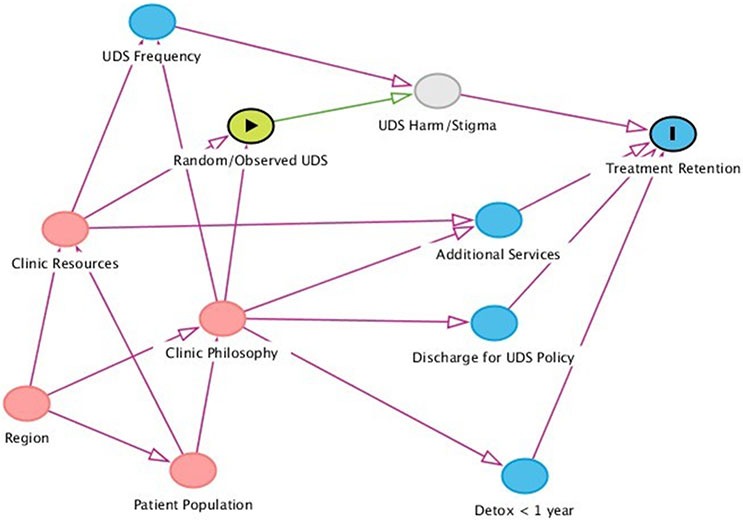
Background: In the US, opioid treatment providers (OTPs) have wide latitude to perform urine drug screening (UDS) and discharge clients for positive results. OTP clients have identified randomized and directly observed UDS as potentially stigmatizing, but little research has examined the association between UDS modality and retention in OTPs.
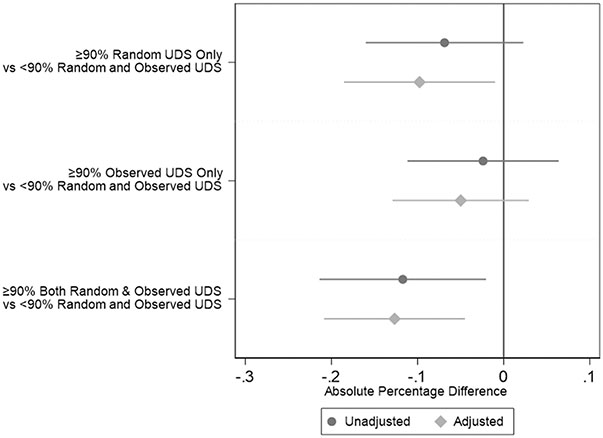
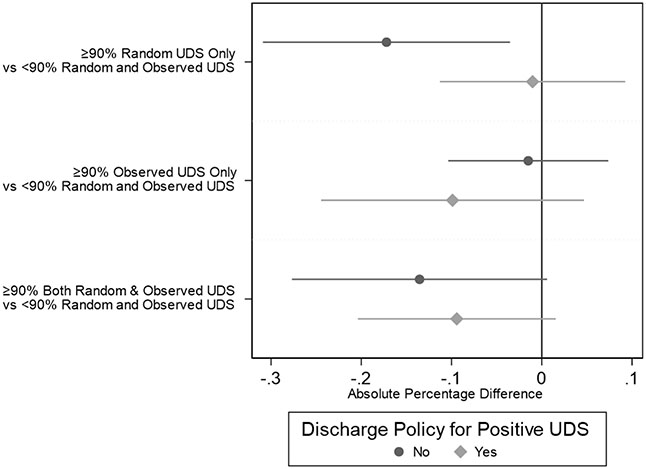
Methods: This cross-sectional study uses the 2016-2017 NDATSS wave among OTPs that administered methadone. The exposure was a 4-level variable based on whether OTPs had a high percentage (≥ 90% of clients) who experienced randomized, observed, both, or neither modality of UDS. The outcome was the proportion of clients retained in treatment 1 year or longer (long-term retention). Analyses were conducted using fractional logit regression with survey weighting and presented as percentages and 95% confidence intervals. We also present how policies for involuntary clinic discharge modify these effects.
Results: 150 OTPs were eligible with a median of 310 clients. 40 (27%) OTPs did not highly utilize either randomized or observed UDS, 22 (15%) only highly utilized observed UDS, 42 (28%) only highly utilized randomized UDS and 46 (31%) utilized both practices on ≥ 90% of clients. Adjusted estimates for long-term retention ranged from 57.7% in OTPs that conducted both randomized and observed UDS on ≥ 90% of clients and 70.4% in OTPs that did not highly utilize these practices. Involuntary discharge may moderate this relationship.
Conclusion: Findings showed an association between high utilization of randomized and observed UDS and decreased long-term retention, suggesting that UDS modality may impact long-term OTP retention.
Keywords: Methadone; Methadone policy; Person-centered treatment; Retention; Stigma; Urine drug screening.
Copyright © 2023. Published by Elsevier B.V.
Conflict of interest statement
Declaration of Competing Interest The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Pryce S. Michener reports financial support was provided by National Institute on Drug Abuse.
Figures
Similar articles
-
Characteristics and current clinical practices of opioid treatment programs in the United States.Drug Alcohol Depend. 2019 Dec 1;205:107616. doi: 10.1016/j.drugalcdep.2019.107616. Epub 2019 Oct 17. Drug Alcohol Depend. 2019. PMID: 31678836
-
Baseline risk factors for drug use among African-American patients during first-month induction/stabilization on methadone.J Subst Abuse Treat. 2017 Jul;78:15-21. doi: 10.1016/j.jsat.2017.04.007. Epub 2017 Apr 14. J Subst Abuse Treat. 2017. PMID: 28554598
-
Associations Between Buprenorphine\Naloxone and Methadone Treatment and non-Opioid Substance Use in Prescription-Type Opioid Use Disorder: Secondary Analyses From the OPTIMA Study: Associations entre le traitement avec la buprénorphine/naloxone et avec la méthadone et l'utilisation de substances non opioïdes dans le trouble lié à l'usage d'opioïdes de type sur ordonnance : analyses secondaires de l'étude OPTIMA.Can J Psychiatry. 2024 Apr;69(4):252-263. doi: 10.1177/07067437231210796. Epub 2023 Oct 30. Can J Psychiatry. 2024. PMID: 37899716 Free PMC article. Clinical Trial.
-
Trends in the Use of Methadone and Buprenorphine at Substance Abuse Treatment Facilities: 2003 to 2011.2013 Apr 23. In: The CBHSQ Report. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2013–. 2013 Apr 23. In: The CBHSQ Report. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2013–. PMID: 27606405 Free Books & Documents. Review.
-
Payment-related barriers to medications for opioid use disorder: A critical review of the literature and real-world application.J Subst Use Addict Treat. 2024 Oct;165:209441. doi: 10.1016/j.josat.2024.209441. Epub 2024 Jun 19. J Subst Use Addict Treat. 2024. PMID: 38906417 Free PMC article. Review.
Cited by
-
Opioid medication doses among safer supply clients: Current safer supply doses and previous OAT experience.Drug Alcohol Depend Rep. 2025 Apr 23;15:100338. doi: 10.1016/j.dadr.2025.100338. eCollection 2025 Jun. Drug Alcohol Depend Rep. 2025. PMID: 40416078 Free PMC article.
-
"Tethered to this ball and chain": Women's perspectives on bodily agency within opioid treatment programs.Int J Drug Policy. 2024 Dec;134:104645. doi: 10.1016/j.drugpo.2024.104645. Epub 2024 Nov 19. Int J Drug Policy. 2024. PMID: 39566258
-
Perceptions of structural and provider-based substance use stigma interventions among primary care professionals.Drug Alcohol Depend Rep. 2024 Jul 14;12:100259. doi: 10.1016/j.dadr.2024.100259. eCollection 2024 Sep. Drug Alcohol Depend Rep. 2024. PMID: 39108608 Free PMC article.
-
Exploring the role of urine drug screening in opioid agonist therapy.Med J Aust. 2025 May 5;222(8):381-383. doi: 10.5694/mja2.52628. Epub 2025 Mar 5. Med J Aust. 2025. PMID: 40043364 Free PMC article. No abstract available.
-
Patient centered medication treatment for opioid use disorder in rural Vermont: a qualitative study.Addict Sci Clin Pract. 2025 Jan 14;20(1):3. doi: 10.1186/s13722-024-00529-8. Addict Sci Clin Pract. 2025. PMID: 39810273 Free PMC article.
References
-
- Adams T., 2005. Outpatient Substance Abuse Treatment Surveys (OSATSS) sampling and weighting documentation for OSATSS-6, 2004. Surv. Res. Cent. Inst. Soc. Res. Ann Harb. Univ. Mich
-
- Adams T, Heeringa S, 2001. Outpatient Substance Abuse Treatment System Survey: Technical Documentation for OSATSS-5, 1999-2000. Ann Arbor MI Inst. Soc. Res
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
