

Glioblastoma vaccines: past, present, and opportunities
- PMID: 38183840
- PMCID: PMC10808938
- DOI: 10.1016/j.ebiom.2023.104963
Glioblastoma vaccines: past, present, and opportunities
Abstract
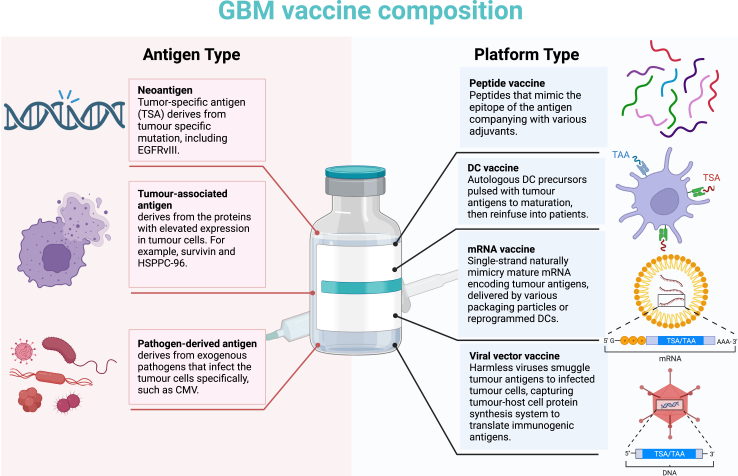
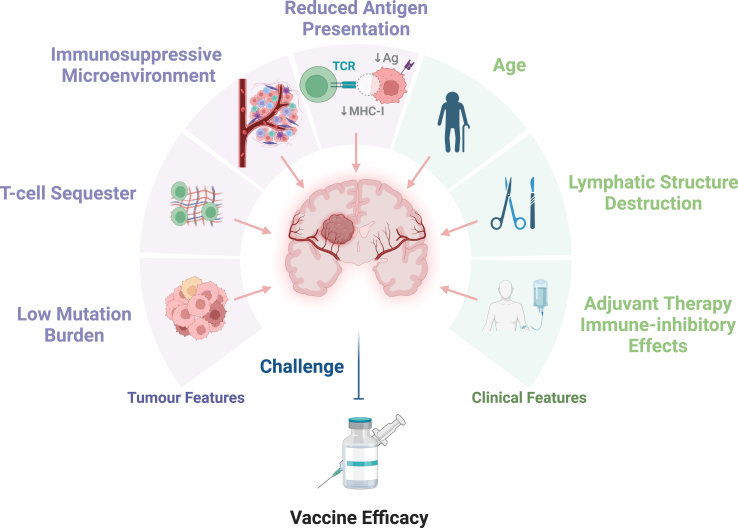
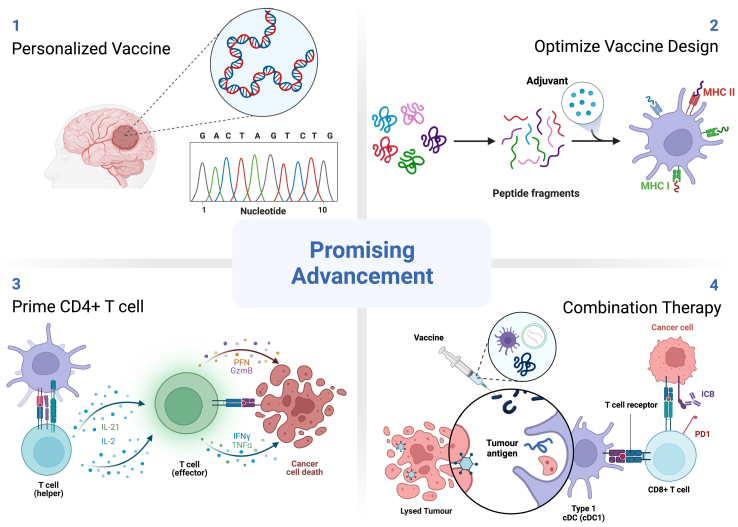
Glioblastoma (GBM) is one of the most lethal central nervous systems (CNS) tumours in adults. As supplements to standard of care (SOC), various immunotherapies improve the therapeutic effect in other cancers. Among them, tumour vaccines can serve as complementary monotherapy or boost the clinical efficacy with other immunotherapies, such as immune checkpoint blockade (ICB) and chimeric antigen receptor T cells (CAR-T) therapy. Previous studies in GBM therapeutic vaccines have suggested that few neoantigens could be targeted in GBM due to low mutation burden, and single-peptide therapeutic vaccination had limited efficacy in tumour control as monotherapy. Combining diverse antigens, including neoantigens, tumour-associated antigens (TAAs), and pathogen-derived antigens, and optimizing vaccine design or vaccination strategy may help with clinical efficacy improvement. In this review, we discussed current GBM therapeutic vaccine platforms, evaluated and potential antigenic targets, current challenges, and perspective opportunities for efficacy improvement.
Keywords: Glioblastoma; Tumour antigen; Vaccine efficacy; Vaccine perspective; Vaccine platform.
Copyright © 2023 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests All authors have nothing to disclosure.
Figures
Similar articles
-
Emerging immunotherapies for glioblastoma.Expert Opin Emerg Drugs. 2016 Jun;21(2):133-45. doi: 10.1080/14728214.2016.1186643. Expert Opin Emerg Drugs. 2016. PMID: 27223671 Free PMC article. Review.
-
Immunotherapy as a New Therapeutic Approach for Brain and Spinal Cord Tumors.Adv Exp Med Biol. 2023;1394:73-84. doi: 10.1007/978-3-031-14732-6_5. Adv Exp Med Biol. 2023. PMID: 36587382
-
Neoantigen discovery and applications in glioblastoma: An immunotherapy perspective.Cancer Lett. 2022 Dec 1;550:215945. doi: 10.1016/j.canlet.2022.215945. Epub 2022 Oct 7. Cancer Lett. 2022. PMID: 36216148 Review.
-
Current Immunotherapies for Glioblastoma Multiforme.Front Immunol. 2021 Mar 9;11:603911. doi: 10.3389/fimmu.2020.603911. eCollection 2020. Front Immunol. 2021. PMID: 33767690 Free PMC article. Review.
-
mRNA-based precision targeting of neoantigens and tumor-associated antigens in malignant brain tumors.Genome Med. 2024 Jan 25;16(1):17. doi: 10.1186/s13073-024-01281-z. Genome Med. 2024. PMID: 38268001 Free PMC article.
Cited by
-
Immunotherapeutic advances in glioma management: The rise of vaccine-based approaches.CNS Neurosci Ther. 2024 Sep;30(9):e70013. doi: 10.1111/cns.70013. CNS Neurosci Ther. 2024. PMID: 39215399 Free PMC article. Review.
-
Co-expression of immune checkpoints in glioblastoma revealed by single-nucleus RNA sequencing and spatial transcriptomics.Comput Struct Biotechnol J. 2024 Apr 10;23:1534-1546. doi: 10.1016/j.csbj.2024.04.014. eCollection 2024 Dec. Comput Struct Biotechnol J. 2024. PMID: 38633388 Free PMC article.
-
Immunotherapy for pediatric low-grade gliomas.Childs Nerv Syst. 2024 Oct;40(10):3263-3275. doi: 10.1007/s00381-024-06491-9. Epub 2024 Jun 17. Childs Nerv Syst. 2024. PMID: 38884777 Review.
-
Trends in the immunotherapy for glioblastoma: A two-decade bibliometric analysis.Hum Vaccin Immunother. 2025 Dec;21(1):2466299. doi: 10.1080/21645515.2025.2466299. Epub 2025 Feb 14. Hum Vaccin Immunother. 2025. PMID: 39950580 Free PMC article.
-
Immuno-oncological interactions between meningeal lymphatics and glioblastoma: from mechanisms to therapies.Theranostics. 2025 Jun 9;15(14):6983-7000. doi: 10.7150/thno.111972. eCollection 2025. Theranostics. 2025. PMID: 40585979 Free PMC article. Review.
References
-
- Stupp R., Mason W.P., van den Bent M.J., et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Weller M., van den Bent M., Hopkins K., et al. EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol. 2014;15(9):e395–e403. - PubMed
-
- Stupp R., Hegi M.E., Mason W.P., et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(5):459–466. - PubMed
-
- Rapp M., Baernreuther J., Turowski B., Steiger H.J., Sabel M., Kamp M.A. Recurrence pattern analysis of primary glioblastoma. World Neurosurg. 2017;103:733–740. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
