

Severe CNS involvement in a subset of long-term treated children with infantile-onset Pompe disease
- PMID: 38184429
- PMCID: PMC11080415
- DOI: 10.1016/j.ymgme.2023.108119
Severe CNS involvement in a subset of long-term treated children with infantile-onset Pompe disease
Abstract
Introduction: The standard of care for patients with infantile-onset Pompe disease (IOPD) is enzyme replacement therapy (ERT), which does not cross the blood brain barrier. While neuromuscular manifestations of IOPD are well-described, central nervous system (CNS) manifestations of this disorder are far less characterized. Here we describe severe CNS-related neurological manifestations including seizures and encephalopathy in six individuals with IOPD.
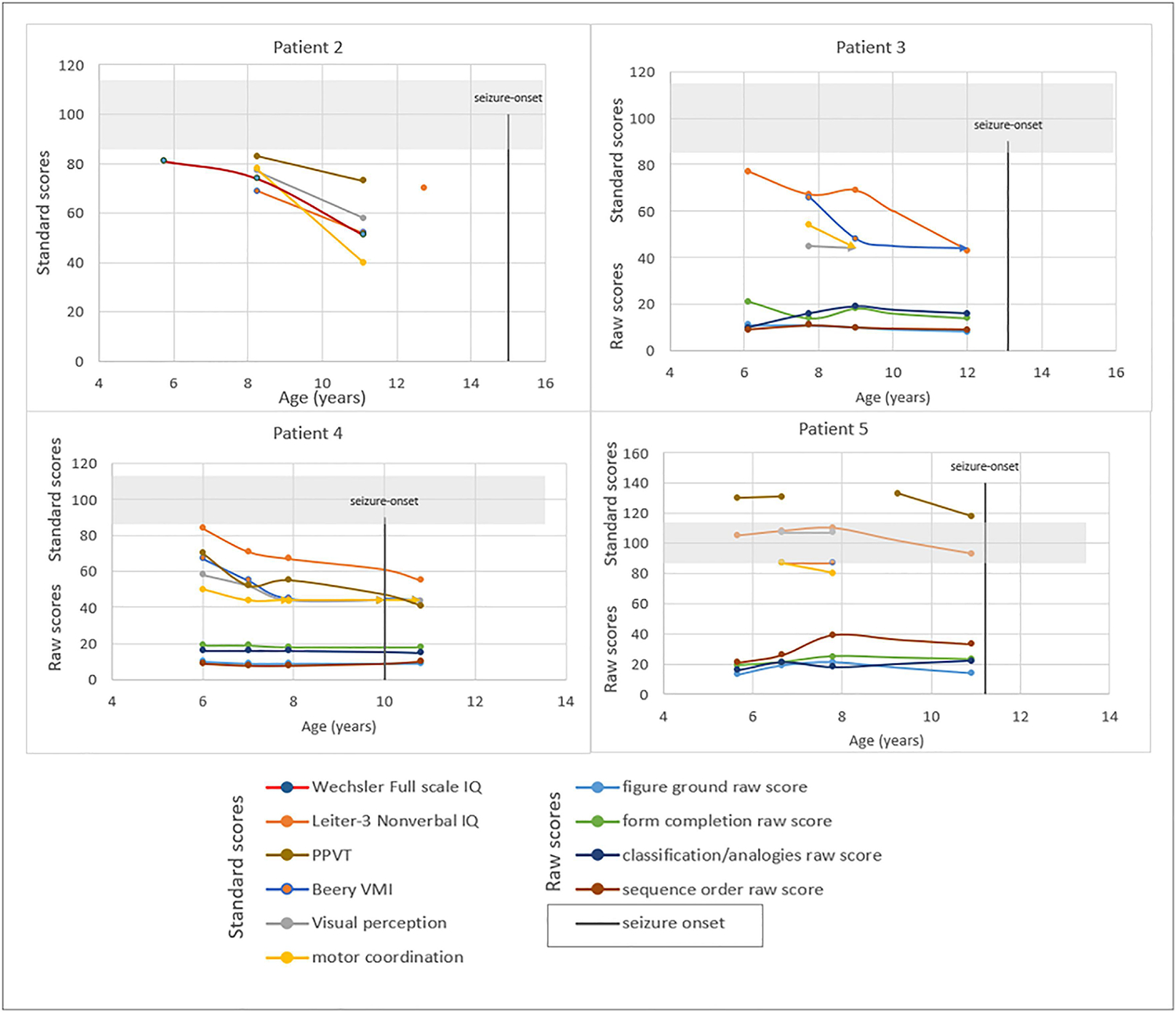
Method: We identified six children with IOPD who developed CNS manifestations such as seizures and/or encephalopathy. We studied their brain magnetic resonance imaging scans (MRIs) and graded the severity of white matter hyperintensities (WMHI) using the Fazekas scale scoring system as previously published. Longitudinal cognitive measures were available from 4/6 children.
Results: All six IOPD patients (4 males/2 females) had been treated with ERT for 12-15 years. Seizures and/or encephalopathy were noted at a median age at onset of 11.9 years (range 9-15 years). All were noted to have extensive WMHI in the brain MRIs and very high Fazekas scores which preceded the onset of neurological symptoms. Longitudinal IQ scores from four of these children suggested developmental plateauing.
Discussion: Among a subset of IOPD patients on long-term ERT, CNS manifestations including hyperreflexia, encephalopathy and seizures may become prominent, and there is likely an association between these symptoms and significant WMHI on MRI. Further study is needed to identify risk factors for CNS deterioration among children with IOPD and develop interventions to prevent neurological decline.
Keywords: Case series; Epilepsy; Pompe disease; White matter disease.
Copyright © 2023. Published by Elsevier Inc.
Conflict of interest statement
Declaration of Competing Interest D. Kenney-Jung, A. Korlimarla, G. A. Spiridigliozzi, M. Malinzak, G. Nichting, S.-H. Jung, C. Phornphutkul and J. Owen report no disclosures. W. F. Wiggins is a Strategic Advisor to Qure.ai. He has served on the Medical Advisory Board of the University of Wisconsin-GE CT Protocols Partnership. A. Sun receives research funding and clinical trial support from Ultragenyx, LogicBio, BioMarin, Aeglea, and Takeda. R. Wang receives research/grant support from Biomarin Pharmaceuticals and Ultragenyx, has received consulting fees / honoraria from Biomarin Pharmaceuticals, Takeda, and Regenxbio Inc., and owns equity in Biomarin Pharmaceuticals and Regenxbio, Inc. J. M. Provenzale receives research funding from Bayer, Inc. P. S. Kishnani has received research/grant support from Sanofi Genzyme and Amicus Therapeutics. She has received consulting fees and honoraria from Sanofi Genzyme, Amicus Therapeutics, Maze Therapeutics, Bayer and Asklepios Biopharmaceutical, Inc. (AskBio). She is a member of the Pompe and Gaucher Disease Registry Advisory Board for Sanofi Genzyme, Pompe Disease Advisory Board for Amicus Therapeutics, and Advisory Board for Baebies. P. S. Kishnani has equity in Asklepios Biopharmaceutical, Inc. (AskBio) and Maze Therapeutics.
Figures

Similar articles
-
Enzyme replacement therapy for infantile-onset Pompe disease.Cochrane Database Syst Rev. 2017 Nov 20;11(11):CD011539. doi: 10.1002/14651858.CD011539.pub2. Cochrane Database Syst Rev. 2017. PMID: 29155436 Free PMC article.
-
Enzyme replacement therapy for late-onset Pompe disease.Cochrane Database Syst Rev. 2023 Dec 12;12(12):CD012993. doi: 10.1002/14651858.CD012993.pub2. Cochrane Database Syst Rev. 2023. PMID: 38084761 Free PMC article.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
Cited by
-
Advances in Pompe Disease Treatment: From Enzyme Replacement to Gene Therapy.Mol Diagn Ther. 2024 Nov;28(6):703-719. doi: 10.1007/s40291-024-00733-x. Epub 2024 Aug 12. Mol Diagn Ther. 2024. PMID: 39134822 Review.
-
Results of orthodontic procedure in a patient with classic infantile Pompe disease.Ital J Pediatr. 2025 Jul 15;51(1):231. doi: 10.1186/s13052-025-02023-6. Ital J Pediatr. 2025. PMID: 40660301 Free PMC article.
-
Expanding therapeutic options for Pompe disease: a new small molecule inhibitor of glycogen synthase 1 (GYS1) shows preclinical promise in Pompe disease.Ann Transl Med. 2024 Dec 24;12(6):123. doi: 10.21037/atm-24-135. Epub 2024 Nov 15. Ann Transl Med. 2024. PMID: 39817232 Free PMC article. No abstract available.
-
Neurological glycogen storage diseases and emerging therapeutics.Neurotherapeutics. 2024 Sep;21(5):e00446. doi: 10.1016/j.neurot.2024.e00446. Epub 2024 Sep 14. Neurotherapeutics. 2024. PMID: 39277505 Free PMC article. Review.
-
Management of Pompe disease alongside and beyond ERT: a narrative review.Acta Myol. 2025 Mar;44(1):11-22. doi: 10.36185/2532-1900-1106. Acta Myol. 2025. PMID: 40183436 Free PMC article. Review.
References
-
- Desai AK, Baloh CH, Sleasman JW, Rosenberg AS, Kishnani PS. Benefits of Prophylactic Short-Course Immune Tolerance Induction in Patients With Infantile Pompe Disease: Demonstration of Long-Term Safety and Efficacy in an Expanded Cohort. Frontiers in Immunology. 2020;11(1727). doi:10.3389/fimmu.2020.01727 - DOI - PMC - PubMed
-
- Li C, Desai AK, Gupta P, et al. Transforming the clinical outcome in CRIM-negative infantile Pompe disease identified via newborn screening: the benefits of early treatment with enzyme replacement therapy and immune tolerance induction. Genetics in Medicine. Published online January 25, 2021. doi:10.1038/s41436-020-01080-y - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
