

The effects of higher versus lower protein delivery in critically ill patients: an updated systematic review and meta-analysis of randomized controlled trials with trial sequential analysis
- PMID: 38184658
- PMCID: PMC10770947
- DOI: 10.1186/s13054-023-04783-1
The effects of higher versus lower protein delivery in critically ill patients: an updated systematic review and meta-analysis of randomized controlled trials with trial sequential analysis
Abstract
Background: A recent large multicentre trial found no difference in clinical outcomes but identified a possibility of increased mortality rates in patients with acute kidney injury (AKI) receiving higher protein. These alarming findings highlighted the urgent need to conduct an updated systematic review and meta-analysis to inform clinical practice.
Methods: From personal files, citation searching, and three databases searched up to 29-5-2023, we included randomized controlled trials (RCTs) of adult critically ill patients that compared higher vs lower protein delivery with similar energy delivery between groups and reported clinical and/or patient-centred outcomes. We conducted random-effect meta-analyses and subsequently trial sequential analyses (TSA) to control for type-1 and type-2 errors. The main subgroup analysis investigated studies with and without combined early physical rehabilitation intervention. A subgroup analysis of AKI vs no/not known AKI was also conducted.
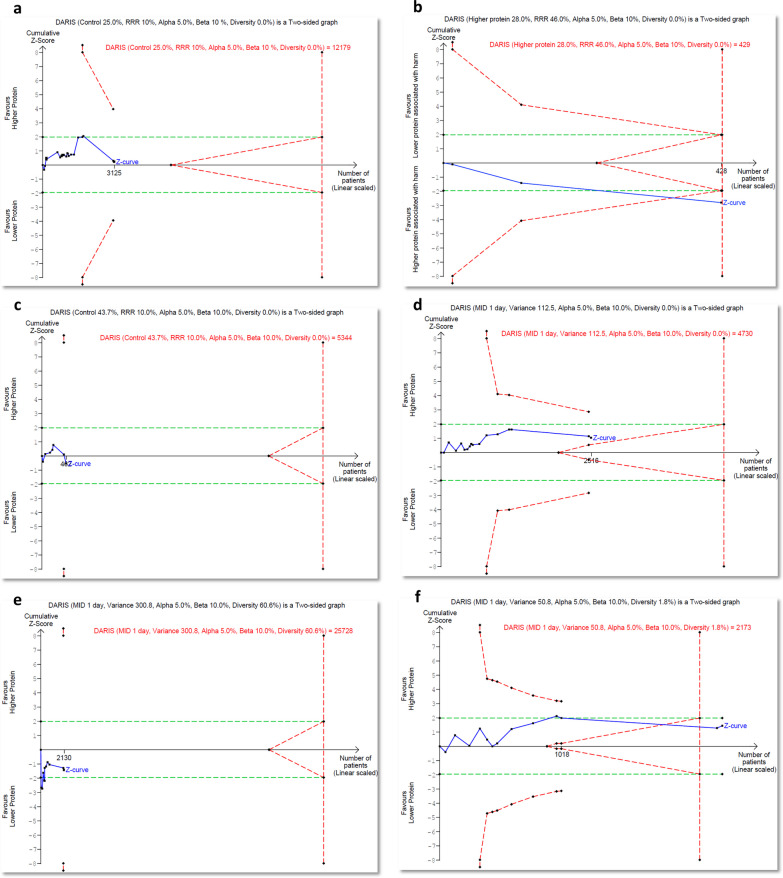
Results: Twenty-three RCTs (n = 3303) with protein delivery of 1.49 ± 0.48 vs 0.92 ± 0.30 g/kg/d were included. Higher protein delivery was not associated with overall mortality (risk ratio [RR]: 0.99, 95% confidence interval [CI] 0.88-1.11; I2 = 0%; 21 studies; low certainty) and other clinical outcomes. In 2 small studies, higher protein combined with early physical rehabilitation showed a trend towards improved self-reported quality-of-life physical function measurements at day-90 (standardized mean difference 0.40, 95% CI - 0.04 to 0.84; I2 = 30%). In the AKI subgroup, higher protein delivery significantly increased mortality (RR 1.42, 95% CI 1.11-1.82; I2 = 0%; 3 studies; confirmed by TSA with high certainty, and the number needed to harm is 7). Higher protein delivery also significantly increased serum urea (mean difference 2.31 mmol/L, 95% CI 1.64-2.97; I2 = 0%; 7 studies).
Conclusion: Higher, compared with lower protein delivery, does not appear to affect clinical outcomes in general critically ill patients but may increase mortality rates in patients with AKI. Further investigation of the combined early physical rehabilitation intervention in non-AKI patients is warranted.
Prospero id: CRD42023441059.
Keywords: Critical illness; Physical rehabilitation; Protein; Systematic review.
© 2024. The Author(s).
Conflict of interest statement
ED has received speaker honoraria from Baxter; AH received stipend from Medical Faculty RWTH Aachen (“Habilitationsstipendium”), grants for IITs from DFG and Fresenius Kabi, Lecture fees, and travel honoraria from Fresenius Kabi and Baxter; AvZ received honoraria for advisory board meetings, lectures, research, and travel expenses from Abbott, AOP Pharma, Baxter, Cardinal Health, Danone-Nutricia, DIM3, Fresenius-Kabi, GE Healthcare, Mermaid, Nestle, Paion, Rousselot, and Lyric; MCGvdP received in kind support from Nutricia Research for the PRECISe trial and speaker and travel fees from Nutricia Research. All other authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
