

Imaging Evaluation of Peritoneal Metastasis: Current and Promising Techniques
- PMID: 38184772
- PMCID: PMC10788608
- DOI: 10.3348/kjr.2023.0840
Imaging Evaluation of Peritoneal Metastasis: Current and Promising Techniques
Abstract
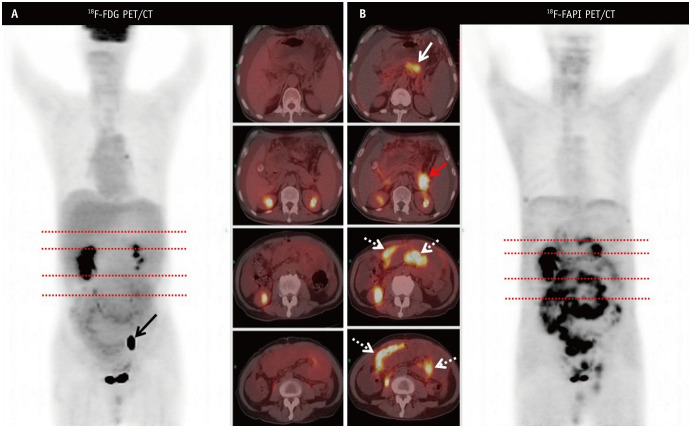
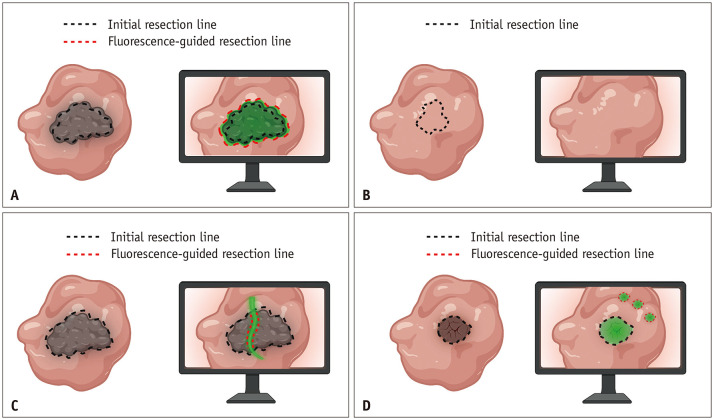
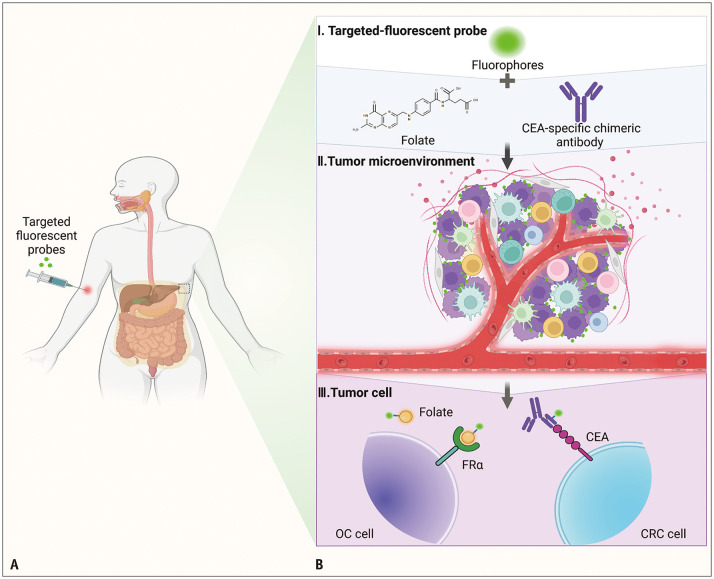
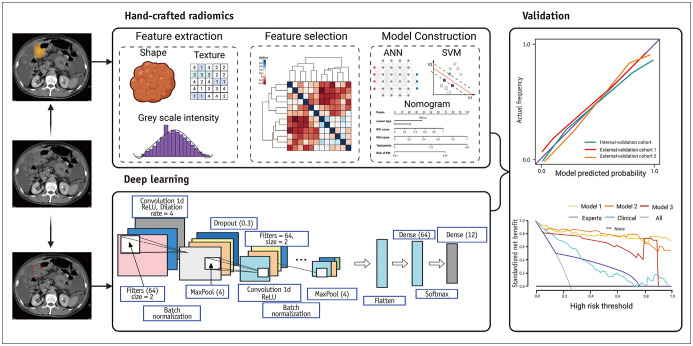
Early diagnosis, accurate assessment, and localization of peritoneal metastasis (PM) are essential for the selection of appropriate treatments and surgical guidance. However, available imaging modalities (computed tomography [CT], conventional magnetic resonance imaging [MRI], and 18fluorodeoxyglucose positron emission tomography [PET]/CT) have limitations. The advent of new imaging techniques and novel molecular imaging agents have revealed molecular processes in the tumor microenvironment as an application for the early diagnosis and assessment of PM as well as real-time guided surgical resection, which has changed clinical management. In contrast to clinical imaging, which is purely qualitative and subjective for interpreting macroscopic structures, radiomics and artificial intelligence (AI) capitalize on high-dimensional numerical data from images that may reflect tumor pathophysiology. A predictive model can be used to predict the occurrence, recurrence, and prognosis of PM, thereby avoiding unnecessary exploratory surgeries. This review summarizes the role and status of different imaging techniques, especially new imaging strategies such as spectral photon-counting CT, fibroblast activation protein inhibitor (FAPI) PET/CT, near-infrared fluorescence imaging, and PET/MRI, for early diagnosis, assessment of surgical indications, and recurrence monitoring in patients with PM. The clinical applications, limitations, and solutions for fluorescence imaging, radiomics, and AI are also discussed.
Keywords: Artificial intelligence; Deep learning; Diagnostic imaging; Machine learning; Molecular imaging; Optical imaging; Peritoneal neoplasms; Radiomics.
Copyright © 2024 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Radiomics in colorectal cancer patients.World J Gastroenterol. 2023 May 21;29(19):2888-2904. doi: 10.3748/wjg.v29.i19.2888. World J Gastroenterol. 2023. PMID: 37274803 Free PMC article. Review.
-
Artificial intelligence applications for oncological positron emission tomography imaging.Eur J Radiol. 2021 Jan;134:109448. doi: 10.1016/j.ejrad.2020.109448. Epub 2020 Nov 30. Eur J Radiol. 2021. PMID: 33307463 Review.
-
18F-FDG PET/CT Radiomics-Based Multimodality Fusion Model for Preoperative Individualized Noninvasive Prediction of Peritoneal Metastasis in Advanced Gastric Cancer.Ann Surg Oncol. 2024 Sep;31(9):6017-6027. doi: 10.1245/s10434-024-15631-z. Epub 2024 Jul 8. Ann Surg Oncol. 2024. PMID: 38976160
-
Usefulness of [68Ga]FAPI-04 and [18F]FDG PET/CT for the detection of primary tumour and metastatic lesions in gastrointestinal carcinoma: a comparative study.Eur Radiol. 2023 Apr;33(4):2779-2791. doi: 10.1007/s00330-022-09251-y. Epub 2022 Nov 17. Eur Radiol. 2023. PMID: 36394603
-
Application of Artificial Intelligence in Oncologic Molecular PET-Imaging: A Narrative Review on Beyond [18F]F-FDG Tracers - Part I. PSMA, Choline, and DOTA Radiotracers.Semin Nucl Med. 2024 Jan;54(1):171-180. doi: 10.1053/j.semnuclmed.2023.08.004. Epub 2023 Sep 24. Semin Nucl Med. 2024. PMID: 37752032 Review.
Cited by
-
Peritoneal Oligometastasis in Gastric Cancer: Diagnostic Strategies, Patient Selection, and Emerging Therapeutic Approaches.J Gastric Cancer. 2025 Jul;25(3):409-423. doi: 10.5230/jgc.2025.25.e36. J Gastric Cancer. 2025. PMID: 40631471 Free PMC article. Review.
-
Characteristics of 18F-FAPI-04 PET/CT in patients with peritoneal metastasis and to predict treatment efficacy, a head-to-head comparison with 18F-FDG PET/CT.Cancer Imaging. 2025 Jun 2;25(1):66. doi: 10.1186/s40644-025-00887-9. Cancer Imaging. 2025. PMID: 40457405 Free PMC article.
-
Laparoscopic surgery is associated with increased risk of postoperative peritoneal metastases in T4 colon cancer: a propensity score analysis.Int J Colorectal Dis. 2025 Jan 2;40(1):2. doi: 10.1007/s00384-024-04773-x. Int J Colorectal Dis. 2025. PMID: 39743636 Free PMC article.
-
Tumor agnostic ultrasmall nanoprobes for fluorescence-guided surgical resection in peritoneal metastasis.Eur J Nucl Med Mol Imaging. 2025 Feb;52(3):1149-1165. doi: 10.1007/s00259-024-06950-0. Epub 2024 Oct 24. Eur J Nucl Med Mol Imaging. 2025. PMID: 39446146
References
-
- Thomassen I, van Gestel YR, van Ramshorst B, Luyer MD, Bosscha K, Nienhuijs SW, et al. Peritoneal carcinomatosis of gastric origin: a population-based study on incidence, survival and risk factors. Int J Cancer. 2014;134:622–628. - PubMed
-
- Klaver YL, Simkens LH, Lemmens VE, Koopman M, Teerenstra S, Bleichrodt RP, et al. Outcomes of colorectal cancer patients with peritoneal carcinomatosis treated with chemotherapy with and without targeted therapy. Eur J Surg Oncol. 2012;38:617–623. - PubMed
-
- Sadeghi B, Arvieux C, Glehen O, Beaujard AC, Rivoire M, Baulieux J, et al. Peritoneal carcinomatosis from non-gynecologic malignancies: results of the EVOCAPE 1 multicentric prospective study. Cancer. 2000;88:358–363. - PubMed
-
- Cortes-Guiral D, Hubner M, Alyami M, Bhatt A, Ceelen W, Glehen O, et al. Primary and metastatic peritoneal surface malignancies. Nat Rev Dis Primers. 2021;7:91. - PubMed
Publication types
MeSH terms
Grants and funding
- 2019PT320005/CAMS
- NHCDP2022028/CAMS
- 2020GSZDSYS02/Key Laboratory of Molecular Diagnostics and Precision Medicine for Surgical Oncology in Gansu Province
- GHB1859/Education Science of Gansu Province
- 2020KCYB-7/GUCM
- 111266548053/Longyuan Youth Innovation and Entrepreneurship Talent Project
- ZHXM-202207/Teaching Research and Reform comprehensive project of Gansu University of Traditional Chinese Medicin
- 22GSSYC-1/Research Fund project of Gansu Provincial Hospital
- 22GSSYB-14/Research Fund project of Gansu Provincial Hospital
LinkOut - more resources
Full Text Sources
Medical
