

Inotuzumab ozogamicin combined with chemotherapy in pediatric B-cell precursor CD22+ acute lymphoblastic leukemia: results of the phase IB ITCC-059 trial
- PMID: 38186333
- PMCID: PMC11443403
- DOI: 10.3324/haematol.2023.284409
Inotuzumab ozogamicin combined with chemotherapy in pediatric B-cell precursor CD22+ acute lymphoblastic leukemia: results of the phase IB ITCC-059 trial
Abstract
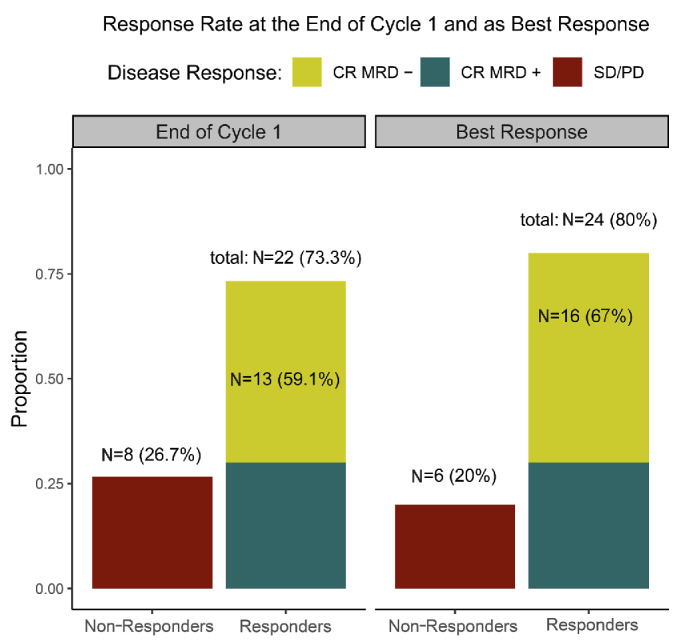
Inotuzumab ozogamicin (InO) is a CD22-directed antibody conjugated with calicheamicin. The phase IB of the ITCC-059 trial tested InO combined with chemotherapy in pediatric B-cell precursor acute lymphoblastic leukemia (BCP-ALL). Relapsed /refractory CD22+ BCP-ALL pediatric patients were enrolled. The primary objective was to establish the recommended phase II dose (RP2D). Secondary objectives included preliminary efficacy and tolerability. InO was combined with 1.5 mg/m2 of vincristine (days 3, 10, 17, 24), 20 mg/m2 of dexamethasone (2 5-day blocks, then amended), and intrathecal therapy. A rolling-6 design was used testing InO from 0.8 to 1.8 mg/m2/cycle. Between May 2020 and April 2022, 30 patients were treated, and 29 were evaluable for dose limiting toxicities (DLT). At 1.1 mg/m2/cycle, two of four patients had DLT (liver toxicity). InO was de-escalated to 0.8 mg/m2/cycle (N=6) without DLT while awaiting a protocol amendment to reduce dexamethasone dose to 10 mg/m2. Post amendment, InO was re-escalated to 1.1 mg/m2/cycle (N=6, 1 DLT), then to 1.4 mg/m2/ cycle (N=3, no DLT), and finally to 1.8 mg/m2/cycle (N=7, 1 DLT). Three additional patients were treated in an expansion cohort. The pooled response rate was 80% (24/30; 95% confidence interval [CI]: 61.4-92.3) and, among responders, 66.7% achieved minimal residual disease negativity. The RP2D of InO combined with vincristine, dexamethasone and intrathecal therapy was declared at 1.8 mg/m2/cycle (1.5 mg/m2/cycle after remission) in a fractioned schedule. This combination showed a response rate similar to the single agent cohorts of this trial, with liver toxicity issues at the initial higher dexamethasone dose (clinicaltrials gov. Identifier: NTR5736).
Figures
References
-
- Rheingold SR, Ji L, Xu X, et al. . Prognostic factors for survival after relapsed acute lymphoblastic leukemia (ALL): a Children’s Oncology Group (COG) study. J Clin Oncol. 2019;37:(Suppl 15):10008.
-
- Von Stackelberg A, Bourquin J-P, Zimmermann M, et al. . ALL-REZ BFM 2002 is associated with improved outcome as compared to ALL-R3 strategy in children with standard risk isolated CNS relapse of acute lymphoblastic leukemia, while maintaining comparable efficacy in patients with bone marrow relapse. results of the multi-national, multi-center Trial IntReALL SR 2010. Blood. 2022;140(Suppl 1):3247-3249.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
