

Efficacy and safety of hypoxia-inducible factor prolyl hydroxylase inhibitors in patients with chronic kidney disease: meta-analysis of phase 3 randomized controlled trials
- PMID: 38186871
- PMCID: PMC10765094
- DOI: 10.1093/ckj/sfad143
Efficacy and safety of hypoxia-inducible factor prolyl hydroxylase inhibitors in patients with chronic kidney disease: meta-analysis of phase 3 randomized controlled trials
Abstract
Background: Hypoxia-inducible factor prolyl hydroxylase inhibitors (HIF-PHIs) are new therapeutic agents for anaemia in chronic kidney disease (CKD). We evaluated by meta-analysis and meta-regression the efficacy and safety of HIF-PHIs in patients with CKD-related anaemia.
Methods: We selected phase 3 randomized clinical trials (RCTs) comparing HIF-PHIs and erythropoiesis-stimulating agents (ESAs) in dialysis and non-dialysis patients. Efficacy outcomes were the changes from baseline of haemoglobin, iron parameters (hepcidin, serum iron, TIBC, TSAT, ferritin) and intravenous iron dose; as safety outcomes we considered cancer, adjudicated major adverse cardiovascular events (MACE), MACE+ (MACE plus hospitalization for hearth failure or unstable angina or thromboembolic event), thrombotic events (deep vein thrombosis, pulmonary embolism), arterovenous fistula (AVF) thrombosis and death.
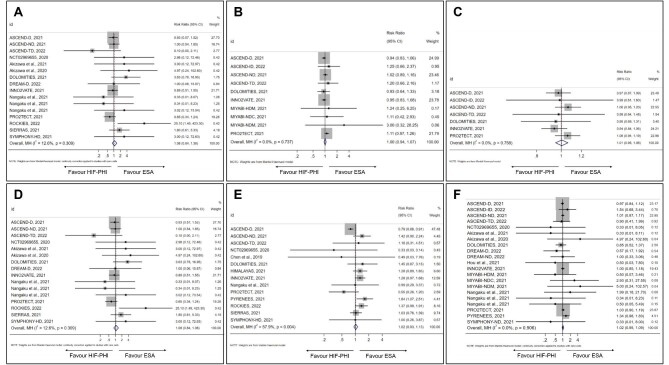
Results: We included 26 RCTs with 24 387 patients. Random effect meta-analysis of the unstandardized mean difference between HIF-PHIs and ESAs showed a significant change in haemoglobin levels from baseline of 0.10 g/dL (95% CI 0.02 to 0.17). Meta-regression analysis showed a significantly higher haemoglobin change for HIF-PHIs in younger patients and versus short-acting ESA (0.21 g/dL, 95% CI 0.12 to 0.29 versus -0.01, 95% CI -0.09 to 0.07 in studies using long-acting ESA, P < .001). No significant effect on heterogeneity was found for type of HIF-PHIs. In comparison with ESAs, HIF-PHIs induced a significant decline in hepcidin and ferritin and a significant increase in serum iron and TIBC, while TSAT did not change; intravenous iron dose was lower with HIF-PHI (-3.1 mg/week, 95% CI -5.6 to -0.6, P = .020). Rate ratio of cancer (0.93, 95% CI 0.76 to 1.13), MACE (1.00, 95% CI 0.94 to 1.07), MACE+ (1.01, 95% CI 0.95 to 1.06), thrombotic events (1.08, 95% CI 0.84 to 1.38), AVF thrombosis (1.02, 95% CI 0.93 to 1.13) and death (1.02, 95% CI 0.95 to 1.13) did not differ between HIF-PHIs and ESAs.
Conclusions: HIF-PHIs at the doses selected for the comparisons are effective in correcting anaemia in comparison with ESA therapy with a significant impact on iron metabolism without notable difference among various agents. No safety signals emerge with use of HIF-PHIs.
Keywords: CKD; HIF-PHI; anemia; haemoglobin; meta-analysis.
© The Author(s) 2023. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
R.M. has been a member of Advisory Boards for Amgen, Astellas and GSK, consulted for Bayer and GSK, and has been an invited speaker at meetings supported by Amgen, Astellas, Vifor Pharma and AstraZeneca. M.E.L.: none. V.S.: none. F.C.S. has been a member of Advisory Boards for Boehringer and Ely-Lilly, and has received fees for scientific consultation and/or lectures by Jansen, Roche Diagnostics, Novo Nordisk, Sanofi, MSD and AstraZeneca. S.B.: none. L.D.N. has received fees for scientific consultation and/or lectures by Amgen, Astellas, AstraZeneca, GSK, Mundibiopharma and Vifor Pharma. C.G.: none.
Figures





References
-
- Johansen KL, Chertow GM, Gilbertson DTet al. US renal data system 2021 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis 2022;79:A8–12. https://doi:10.1053/j.ajkd.2022.02.001. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
