

GAPDH: unveiling its impact as a key hypoxia-related player in head and neck squamous cell carcinoma tumor progression, prognosis, and therapeutic potential
- PMID: 38187058
- PMCID: PMC10767337
GAPDH: unveiling its impact as a key hypoxia-related player in head and neck squamous cell carcinoma tumor progression, prognosis, and therapeutic potential
Abstract
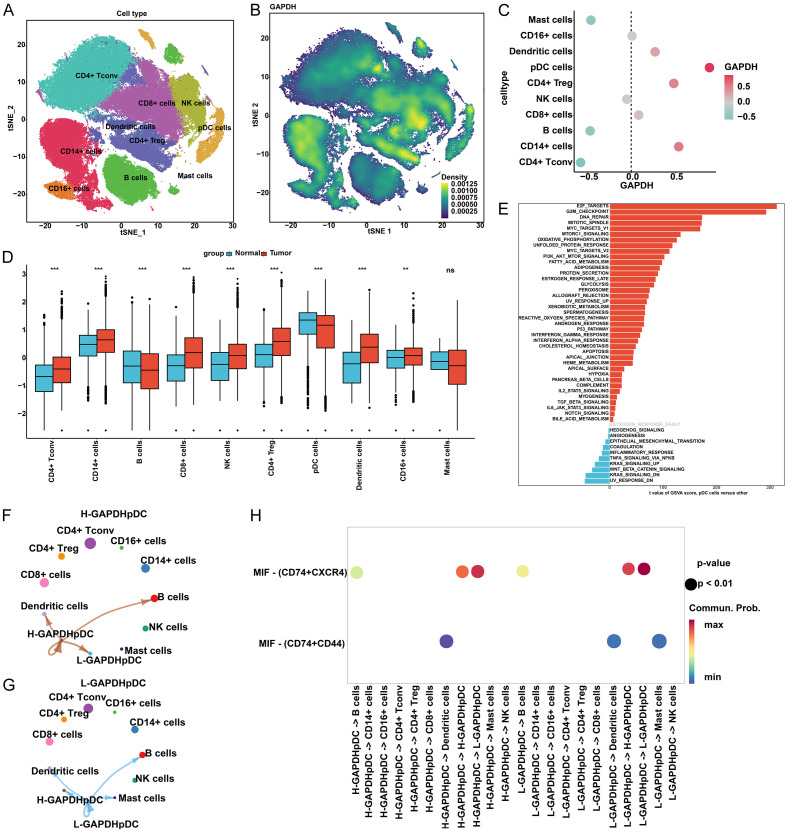
Head and neck squamous cell carcinoma (HNSCC), characterized by hypoxia patterns, ranks as the sixth most prevalent malignant tumor worldwide. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) plays a role in oncogenesis under hypoxic conditions in various cancers. However, its precise function in HNSCC, especially under varied hypoxic conditions, including at high altitudes, remains unclear. Elevated GAPDH mRNA and protein levels in HNSCC relative to normal tissues have been demonstrated through data from The Cancer Genome Atlas (TCGA), GSE29330, and the Human Protein Atlas (P<0.05). This elevation was further confirmed through in vitro experiments utilizing two HNSCC cell lines and a normal oral mucosal epithelial cell line. Additionally, data from TCGA and GSE41613 reveal a correlation between elevated GAPDH expression and diminished overall and progression-free survival in patients (P<0.05). Subsequent analysis identifies GAPDH as an independent risk factor for HNSCC (P<0.05). Using the ESTIMATE and single-sample gene set enrichment analysis (ssGSEA) algorithms, high GAPDH expression was found to be associated with reduced immune scores and diminished anti-tumor cell infiltration, such as CD8+ T cells, in TCGA and GSE41613 datasets (P<0.05). Analysis of single-cell RNA sequencing data from GSE139324 suggests that elevated GAPDH expression hinders communication between plasmacytoid dendritic cells and mast cells (P<0.05). Furthermore, in the TCGA and GSE41613 datasets, GAPDH's biological function is closely tied to hypoxia through Gene Ontology (GO), Kyoto Encyclopedia of Genes and Genomes (KEGG), and Gene Set Variation Analysis (GSVA) analyses. Moreover, its expression is linked to one cuproptosis-related gene, five N6-methyladenosine-related genes, six immune checkpoint genes, and pivotal pathways such as MYC and E2F (P<0.05). GAPDH showed excellent predictive value in estimating the efficacy of immunotherapy and 11 anti-tumor drugs (e.g., cisplatin) (P<0.05), using TIDE and pRRophetic algorithms on the TCGA and GSE41613 datasets. Under 1% O2 in vitro, HNSCC cells show elevated GAPDH expression, leading to decreased apoptosis and increased migration, clonogenicity, invasiveness, and resistance to cisplatin (P<0.05). At 5% O2, these effects persisted, albeit less pronouncedly. Inhibiting GAPDH reversed these effects under all oxygen concentrations (P<0.05). Overall, our findings reveal GAPDH as a key hypoxia-related player influencing tumor progression, prognosis, and therapeutic potential in HNSCC.
Keywords: GAPDH; Hypoxia; cisplatin; head and neck squamous cell carcinoma; immunotherapy.
AJCR Copyright © 2023.
Conflict of interest statement
None.
Figures










Similar articles
-
Identification and verification of eight cancer-associated fibroblasts related genes as a prognostic signature for head and neck squamous cell carcinoma.Heliyon. 2023 Feb 28;9(3):e14003. doi: 10.1016/j.heliyon.2023.e14003. eCollection 2023 Mar. Heliyon. 2023. PMID: 36938461 Free PMC article.
-
A meta-validated immune infiltration-related gene model predicts prognosis and immunotherapy sensitivity in HNSCC.BMC Cancer. 2023 Jan 13;23(1):45. doi: 10.1186/s12885-023-10532-y. BMC Cancer. 2023. PMID: 36639648 Free PMC article.
-
HtrA3: a promising prognostic biomarker and therapeutic target for head and neck squamous cell carcinoma.PeerJ. 2023 Oct 10;11:e16237. doi: 10.7717/peerj.16237. eCollection 2023. PeerJ. 2023. PMID: 37842043 Free PMC article.
-
Targeting exercise-related genes and placental growth factor for therapeutic development in head and neck squamous cell carcinoma.Front Pharmacol. 2024 Oct 4;15:1476076. doi: 10.3389/fphar.2024.1476076. eCollection 2024. Front Pharmacol. 2024. PMID: 39431157 Free PMC article.
-
Role of Vitamin D in Head and Neck Cancer-Immune Function, Anti-Tumour Effect, and Its Impact on Patient Prognosis.Nutrients. 2023 May 31;15(11):2592. doi: 10.3390/nu15112592. Nutrients. 2023. PMID: 37299554 Free PMC article. Review.
Cited by
-
Uncovering gene and cellular signatures of immune checkpoint response via machine learning and single-cell RNA-seq.NPJ Precis Oncol. 2025 Apr 2;9(1):95. doi: 10.1038/s41698-025-00883-z. NPJ Precis Oncol. 2025. PMID: 40169777 Free PMC article.
-
Development of a quantitative genomic instability scoring system and a related competing endogenous RNA network in head and neck squamous cell carcinoma.Transl Cancer Res. 2025 Jul 30;14(7):4115-4141. doi: 10.21037/tcr-24-1925. Epub 2025 Jul 27. Transl Cancer Res. 2025. PMID: 40792171 Free PMC article.
-
T lymphocyte and neutrophil/lymphocyte ratio in patients with radiation-induced oral mucositis after intensity-modulated radiation therapy for head and neck cancer: A retrospective single-center study.Medicine (Baltimore). 2024 May 31;103(22):e38355. doi: 10.1097/MD.0000000000038355. Medicine (Baltimore). 2024. PMID: 39259120 Free PMC article.
-
The Complex Role of Mast Cells in Head and Neck Squamous Cell Carcinoma: A Systematic Review.Medicina (Kaunas). 2024 Jul 19;60(7):1173. doi: 10.3390/medicina60071173. Medicina (Kaunas). 2024. PMID: 39064602 Free PMC article.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
-
- Marur S, Forastiere AA. Head and neck squamous cell carcinoma: update on epidemiology, diagnosis, and treatment. Mayo Clin Proc. 2016;91:386–396. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials