

Prognostic factors affecting long-term outcomes in patients with concurrent IgA nephropathy and membranous nephropathy
- PMID: 38187325
- PMCID: PMC10770449
- DOI: 10.1016/j.heliyon.2023.e23436
Prognostic factors affecting long-term outcomes in patients with concurrent IgA nephropathy and membranous nephropathy
Abstract
Background: The incidence of concurrent immunoglobulin A nephropathy and membranous nephropathy (cIgAN/MN) is low and rarely reported, and the prognosis of patients with cIgAN/MN remains unclear. This study was designed to compare the clinical and prognostic characteristics of cIgAN/MN with IgAN and MN and to identify crucial factors influencing the outcomes of patients with cIgAN/MN.
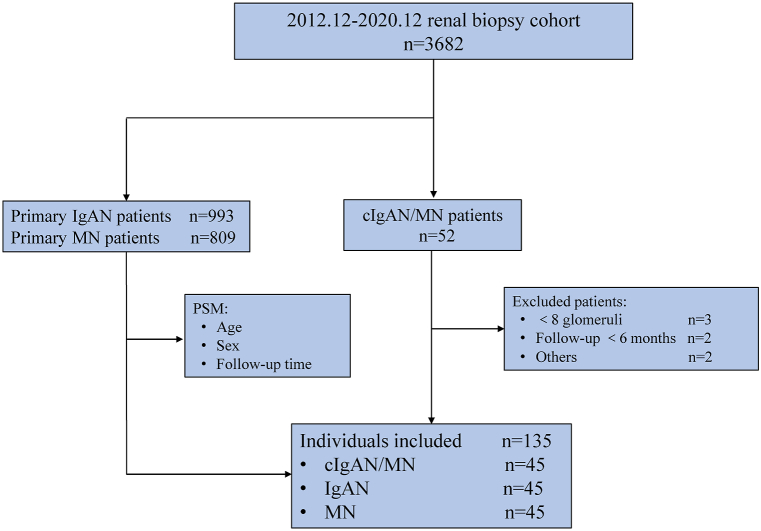
Methods: We included biopsy-proven cIgAN/MN patients between December 2012 and December 2020 at Xijing Hospital. In the same period, propensity score matching was employed to select an equal number of IgAN and MN patients according to the following criteria: age, sex, and follow-up time. The primary endpoint was defined as a composite of eGFR decline ≥30 %, end-stage renal disease, or death. The patient survival rate was examined using Kaplan-Meier survival curves. Univariate and multivariate Cox regression analysis models were utilized to identify the risk factors affecting renal prognosis.
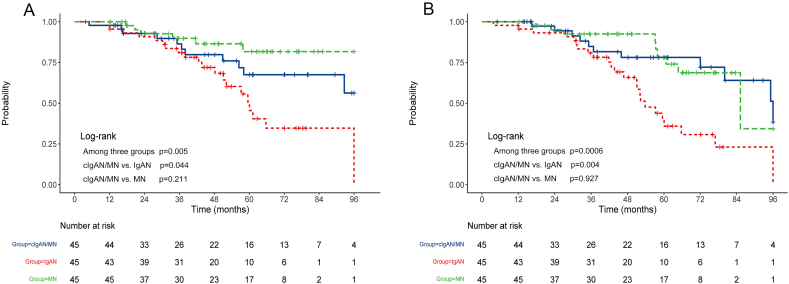
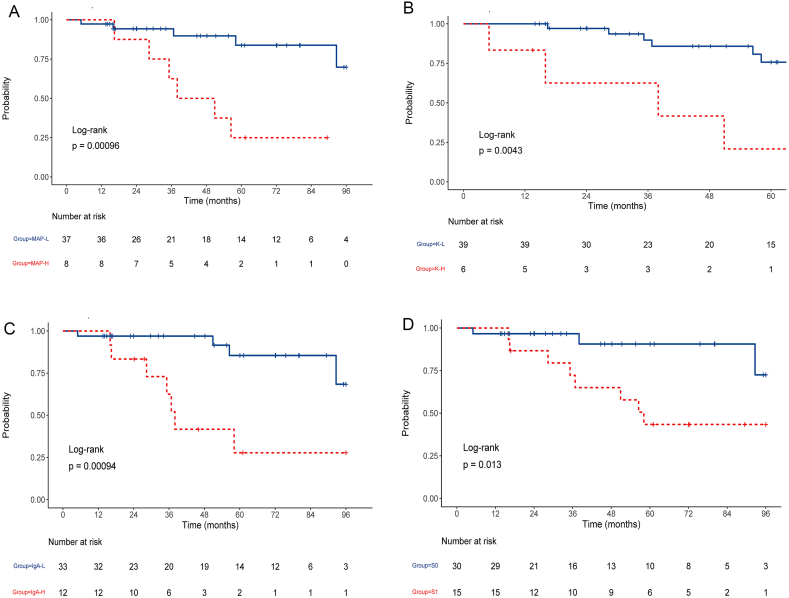
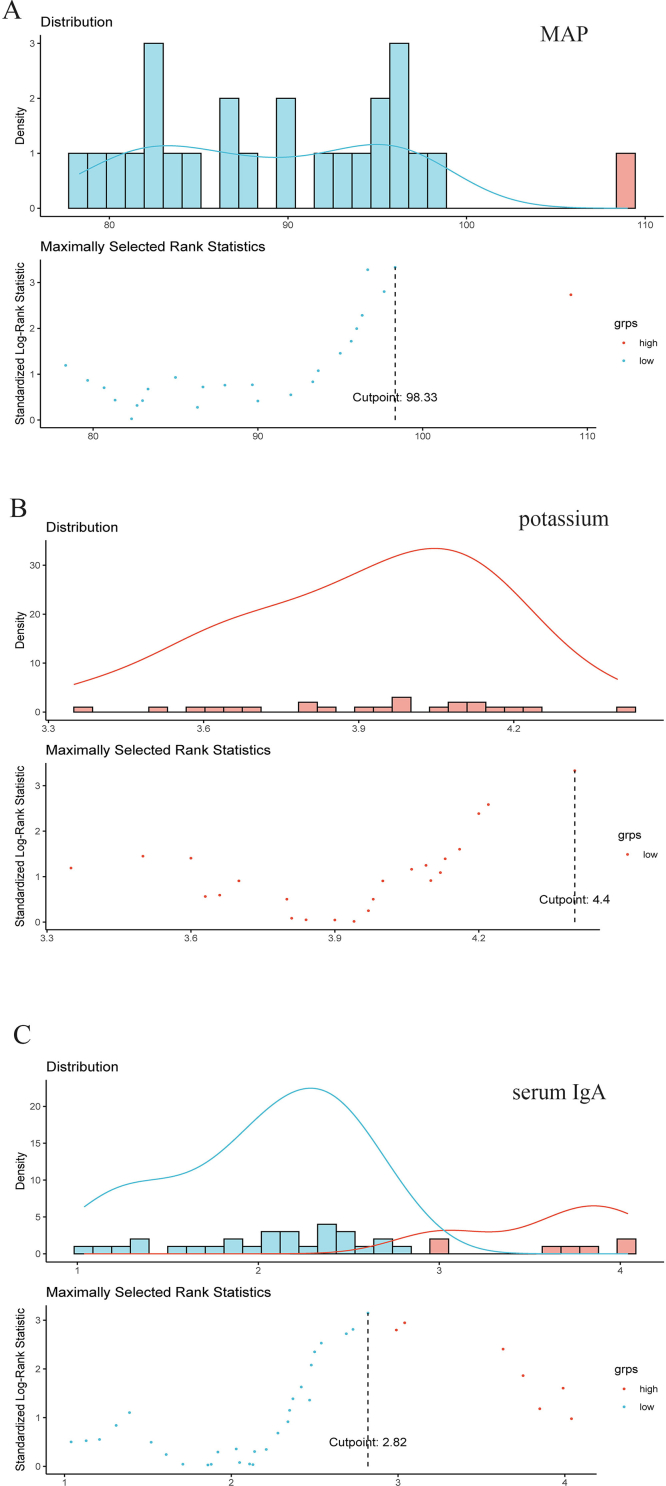
Results: A total of 135 patients were finally included in this study and 35 (25.9 %) reached the primary endpoint. The median follow-up time of cIgAN/MN was 45.9 (24.0, 72.0) months. Compared to the IgAN group, the cIgAN/MN group exhibited a lower cumulative incidence rate of composite renal endpoints (P = 0.044), while no significant difference was found between MN and cIgAN/MN patients (P = 0.211). Univariate Cox analysis revealed that mean arterial pressure, serum potassium, blood urea nitrogen, serum IgA, segmental glomerulosclerosis (S1), and MN staging were associated with an increased risk of renal composite endpoints. The multivariate Cox regression analysis of clinical variables plus histological lesion scoring demonstrated that potassium (HR = 14.350, 95 % CI 2.637-78.090, P = 0.002), serum IgA (HR = 1.870, 95 % CI 1.109-3.153, P = 0.019), and S1 (HR = 11.965, 95 % CI 2.166-66.105, P = 0.004) were independent risk factors influencing renal outcomes in cIgAN/MN patients.
Conclusion: The prognosis of cIgAN/MN patients may exhibit an intermediate pattern between IgAN and MN, leaning towards being more similar to MN in certain aspects. Within the cIgAN/MN cohort, potassium, and serum IgA may be more predictive of rapid progression of renal endpoints, and S1 may indicate a more aggressive disease course.
Keywords: Chronic kidney disease; Concurrent IgAN and MN; Prognostic model; Risk factor.
© 2023 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Concurrent IgA Nephropathy and Membranous Nephropathy, Is It an Overlap Syndrome?Front Immunol. 2022 Mar 11;13:846323. doi: 10.3389/fimmu.2022.846323. eCollection 2022. Front Immunol. 2022. PMID: 35359934 Free PMC article.
-
Clinicopathological analysis of IgA nephropathy combined with other glomerular diseases.Medicine (Baltimore). 2019 Oct;98(41):e17388. doi: 10.1097/MD.0000000000017388. Medicine (Baltimore). 2019. PMID: 31593089 Free PMC article.
-
Divergent manifestations and outcomes of diffuse crescentic immunoglobulin A nephropathy and pauci-immune crescentic glomerulonephritis on long-term.Int Urol Nephrol. 2023 Jul;55(7):1847-1855. doi: 10.1007/s11255-023-03465-9. Epub 2023 Feb 14. Int Urol Nephrol. 2023. PMID: 36781681
-
Clinical and prognostic significance of C1q deposition in IgAN patients-a retrospective study.Int Immunopharmacol. 2020 Nov;88:106896. doi: 10.1016/j.intimp.2020.106896. Epub 2020 Oct 14. Int Immunopharmacol. 2020. PMID: 33182045
-
Pediatric IgA Nephropathy in Europe.Kidney Dis (Basel). 2019 Jun;5(3):182-188. doi: 10.1159/000495751. Epub 2019 Jan 24. Kidney Dis (Basel). 2019. PMID: 31259180 Free PMC article. Review.
Cited by
-
Membranous nephropathy: pathogenesis and treatments.MedComm (2020). 2024 Jun 29;5(7):e614. doi: 10.1002/mco2.614. eCollection 2024 Jul. MedComm (2020). 2024. PMID: 38948114 Free PMC article. Review.
-
Overlap of membranous nephropathy and IgA nephropathy in a patient with Kimura's disease: a case report and literature review.Front Immunol. 2024 Jul 12;15:1404954. doi: 10.3389/fimmu.2024.1404954. eCollection 2024. Front Immunol. 2024. PMID: 39072328 Free PMC article. Review.
-
A case of neuron-derived neurotrophic factor-positive, syphilis-related membranous nephropathy that achieved spontaneous remission.CEN Case Rep. 2025 Jun;14(3):318-323. doi: 10.1007/s13730-024-00960-5. Epub 2024 Dec 28. CEN Case Rep. 2025. PMID: 39733185 Free PMC article.
-
Clinical characteristics, prognosis, and predictive modeling in class IV ± V lupus nephritis.Front Immunol. 2025 May 15;16:1580146. doi: 10.3389/fimmu.2025.1580146. eCollection 2025. Front Immunol. 2025. PMID: 40443677 Free PMC article.
References
-
- Yang C., et al. Executive summary for China kidney disease network (CK-NET) 2016 annual data report. Kidney Int. 2020;98(6):1419–1423. - PubMed
-
- Zhao J., et al. Low-dose corticosteroid combined with mycophenolate mofetil for IgA nephropathy with stage 3 or 4 CKD: a retrospective cohort study. Clin. Therapeut. 2021;43(5):859–870. - PubMed
-
- Doi T., et al. 1983. An Overlapping Syndrome of IgA Nephropathy and Membranous Nephropathy? pp. 24–30. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
