

This is a preprint.
Diroximel fumarate acts through Nrf2 to attenuate methylglyoxal-induced nociception in mice and decreases ISR activation in DRG neurons
- PMID: 38187575
- PMCID: PMC10769417
- DOI: 10.1101/2023.12.22.572877
Diroximel fumarate acts through Nrf2 to attenuate methylglyoxal-induced nociception in mice and decreases ISR activation in DRG neurons
Update in
-
Diroximel Fumarate Acts Through Nrf2 to Attenuate Methylglyoxal-Induced Nociception in Mice and Decrease ISR Activation in DRG Neurons.Diabetes. 2025 May 1;74(5):827-837. doi: 10.2337/db23-1025. Diabetes. 2025. PMID: 39976640 Free PMC article.
Abstract
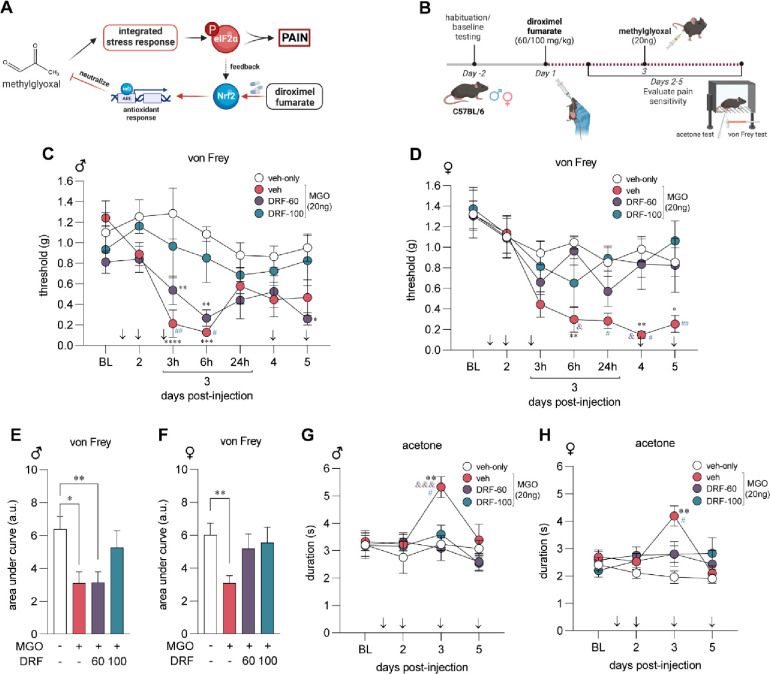
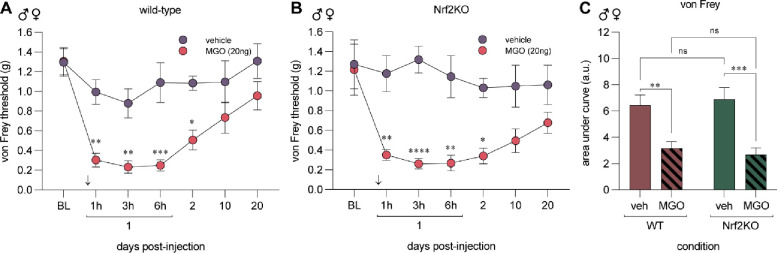
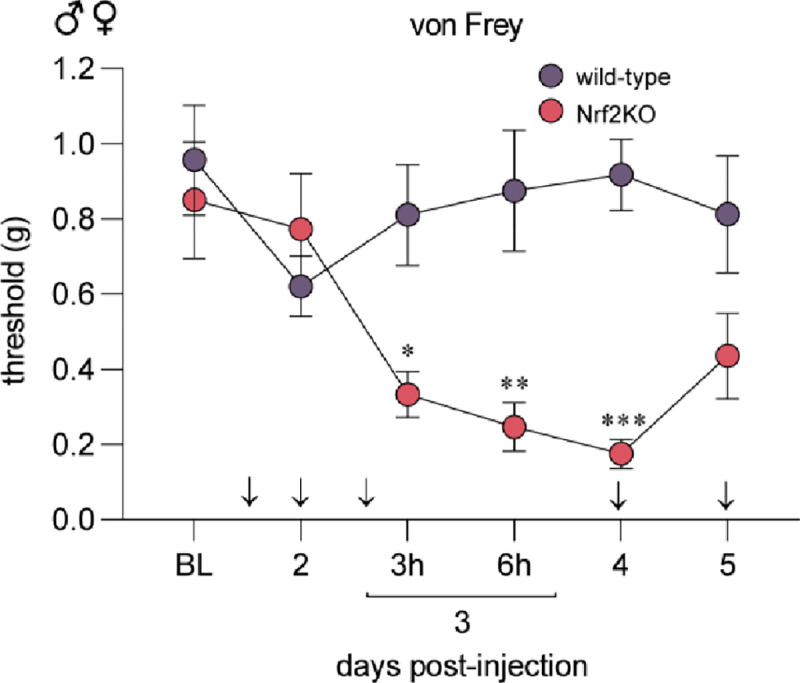
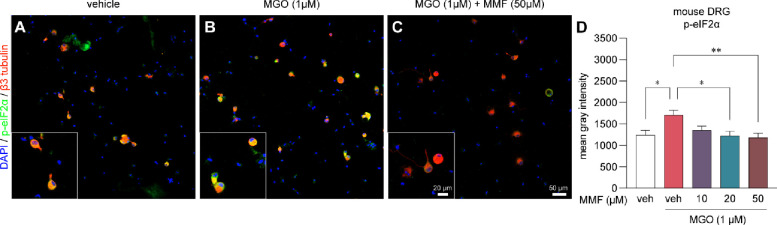
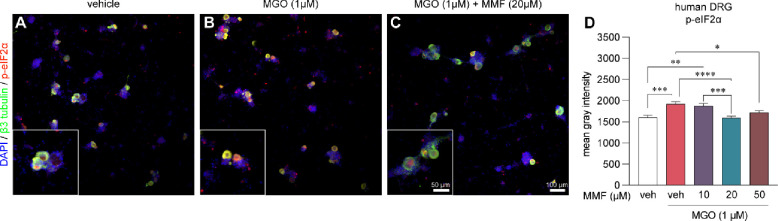
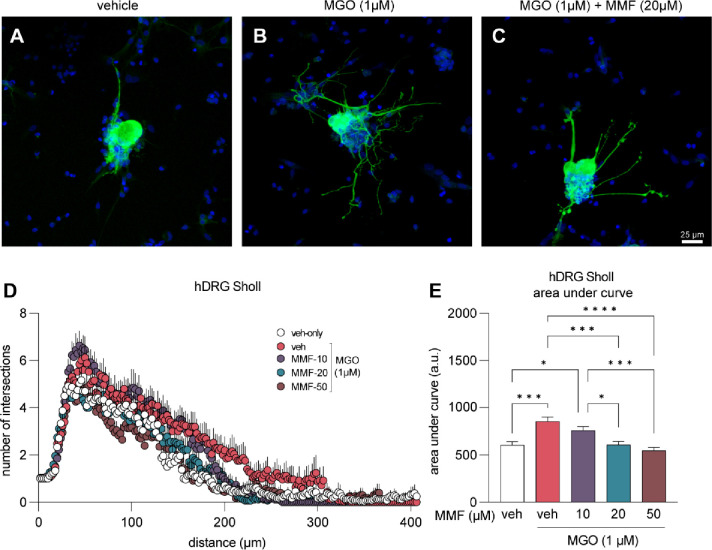
Diabetic neuropathic pain is associated with elevated plasma levels of methylglyoxal (MGO). MGO is a metabolite of glycolysis that causes mechanical hypersensitivity in mice by inducing the integrated stress response (ISR), which is characterized by phosphorylation of eukaryotic initiation factor 2α (p-eIF2α). Nuclear factor erythroid 2-related factor 2 (Nrf2) is a transcription factor that regulates the expression of antioxidant proteins that neutralize MGO. We hypothesized that activating Nrf2 using diroximel fumarate (DRF) would alleviate MGO-induced pain hypersensitivity. We pretreated male and female C57BL/6 mice daily with oral DRF prior to intraplantar injection of MGO (20 ng). DRF (100 mg/kg) treated animals were protected from developing MGO-induced mechanical and cold hypersensitivity. Using Nrf2 knockout mice we demonstrate that Nrf2 is necessary for the anti-nociceptive effects of DRF. In cultured mouse and human dorsal root ganglion (DRG) sensory neurons, we found that MGO induced elevated levels of p-eIF2α. Co-treatment of MGO (1 μM) with monomethyl fumarate (MMF, 10, 20, 50 μM), the active metabolite of DRF, reduced p-eIF2α levels and prevented aberrant neurite outgrowth in human DRG neurons. Our data show that targeting the Nrf2 antioxidant system with DRF is a strategy to potentially alleviate pain associated with elevated MGO levels.
Keywords: Neuroscience; Pharmacology; diroximel fumarate; integrated stress response; methylglyoxal; nrf2; pain.
Conflict of interest statement
Conflict of Interest Statement: PMG received funding from Biogen Inc. and is a founder of ImmunoLogic which is developing Nrf2 directed therapeutics. MSY and TJP are founders of NuvoNuro, a company developing ISR targeted approaches for pain. The other authors declare no conflicts of interest related to this work.
Figures
References
-
- Feldman EL, Callaghan BC, Pop-Busui R, Zochodne DW, Wright DE, Bennett DL, Bril V, Russell JW, Viswanathan V: Diabetic neuropathy. Nat Rev Dis Primers 2019;5:41. - PubMed
-
- McQuay HJ, Tramer M, Nye BA, Carroll D, Wiffen PJ, Moore RA: A systematic review of antidepressants in neuropathic pain. Pain 1996;68:217–227 - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources