

Safety and feasibility of laparoscopic radical resection for bismuth types III and IV hilar cholangiocarcinoma: a single-center experience from China
- PMID: 38188306
- PMCID: PMC10766688
- DOI: 10.3389/fonc.2023.1280513
Safety and feasibility of laparoscopic radical resection for bismuth types III and IV hilar cholangiocarcinoma: a single-center experience from China
Abstract
Background: Surgery represents the only cure for hilar cholangiocarcinoma (HC). However, laparoscopic radical resection remains technically challenging owing to the complex anatomy and reconstruction required during surgery. Therefore, reports on laparoscopic surgery (LS) for HC, especially for types III and IV, are limited. This study aimed to evaluate the safety and feasibility of laparoscopic radical surgery for Bismuth types III and IV HC.
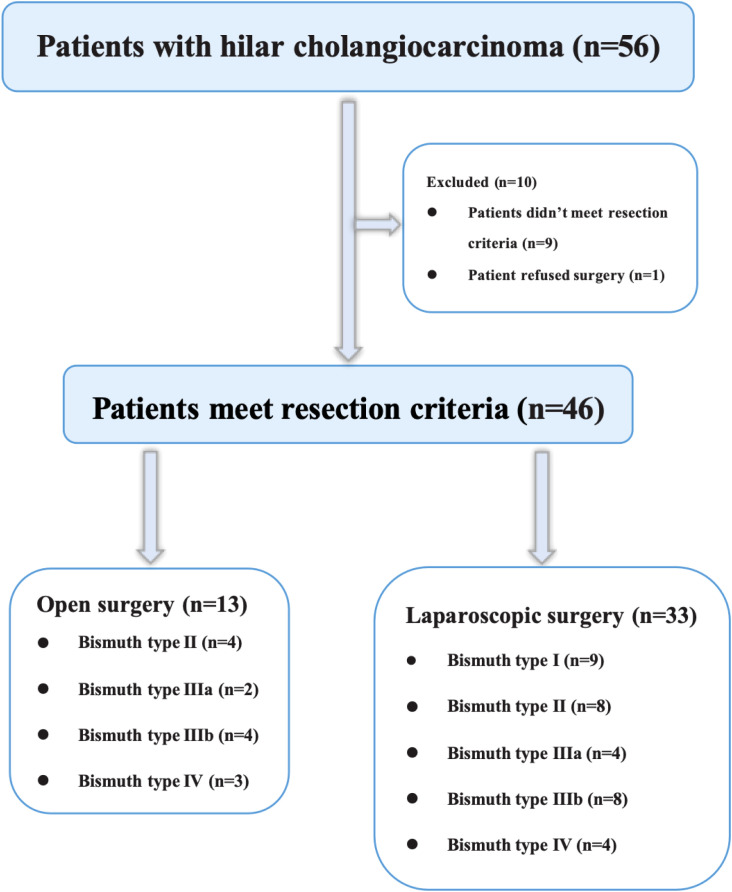
Methods: The data of 16 patients who underwent LS and 9 who underwent open surgery (OS) for Bismuth types III and IV HC at Mianyang Central Hospital, School of Medicine, University of Electronic Science and Technology of China, between December 2017 and January 2022 were analyzed. Basic patient information, Bismuth-Corlette type, AJCC staging, postoperative complications, pathological findings, and follow-up results were evaluated.
Results: Sixteen patients underwent LS and 9 underwent OS for HC. According to the preoperative imaging data, there were four cases of Bismuth type IIIa, eight of type IIIb, and four of type IV in the LS group and two of type IIIa, four of type IIIb, and three of type IV in the OS group (P>0.05). There were no significant differences in age, sex, ASA score, comorbidity, preoperative percutaneous transhepatic biliary drainage rate, history of abdominal surgery, or preoperative laboratory tests between the two groups (P>0.05). Although the mean operative time and mean intraoperative blood loss were higher in the LS group than in OS group, the differences were not statistically significant (P=0.121 and P=0.115, respectively). Four patients (25%) in the LS group and two (22.2%) in the OS group experienced postoperative complications (P>0.05). No significant differences were observed in other surgical outcomes and pathologic findings between the two groups. Regarding the tumor recurrence rate, there was no difference between the groups (P>0.05) during the follow-up period (23.9 ± 13.3 months vs. 17.8 ± 12.3 months, P=0.240).
Conclusion: Laparoscopic radical resection of Bismuth types III and IV HC remains challenging, and extremely delicate surgical skills are required when performing extended hemihepatectomy followed by complex bilioenteric reconstructions. However, this procedure is generally safe and feasible for hepatobiliary surgeons with extensive laparoscopy experience.
Keywords: caudate lobectomy; hilar cholangiocarcinoma; laparoscopy; radical resection; safety.
Copyright © 2023 Wang, Xia, Cao, Zeng, Luo, Cai, Shi, Luo and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
"Hepatic hilum area priority, liver posterior first": An optimized strategy in laparoscopic resection for type III-IV hilar cholangiocarcinoma.World J Gastrointest Surg. 2024 Jul 27;16(7):2167-2174. doi: 10.4240/wjgs.v16.i7.2167. World J Gastrointest Surg. 2024. PMID: 39087123 Free PMC article.
-
Comparison of Efficacy and Safety Between Laparoscopic and Open Radical Resection for Hilar Cholangiocarcinoma-A Propensity Score-Matching Analysis.Front Oncol. 2022 Sep 26;12:1004974. doi: 10.3389/fonc.2022.1004974. eCollection 2022. Front Oncol. 2022. PMID: 36226051 Free PMC article.
-
Total laparoscopic radical resection of hilar cholangiocarcinoma: preliminary experience of a single center.BMC Surg. 2024 Aug 24;24(1):241. doi: 10.1186/s12893-024-02533-w. BMC Surg. 2024. PMID: 39182023 Free PMC article.
-
Robotic Hepatectomy plus Biliary Reconstruction for Bismuth Type III and Type IV Hilar Cholangiocarcinoma: State of the Art and Literature Review.J Pers Med. 2023 Dec 21;14(1):12. doi: 10.3390/jpm14010012. J Pers Med. 2023. PMID: 38276227 Free PMC article. Review.
-
Laparoscopic surgery and robotic surgery for hilar cholangiocarcinoma: an updated systematic review.ANZ J Surg. 2021 Jan;91(1-2):42-48. doi: 10.1111/ans.15948. Epub 2020 May 12. ANZ J Surg. 2021. PMID: 32395906
References
LinkOut - more resources
Full Text Sources