

Intraductal radiofrequency ablation plus biliary stent versus stent alone for malignant biliary obstruction: a systematic review and meta-analysis
- PMID: 38188927
- PMCID: PMC10769587
- DOI: 10.1055/a-2204-8316
Intraductal radiofrequency ablation plus biliary stent versus stent alone for malignant biliary obstruction: a systematic review and meta-analysis
Erratum in
-
Correction: Intraductal radiofrequency ablation plus biliary stent versus stent alone for malignant biliary obstruction: a systematic review and meta-analysis.Endosc Int Open. 2024 Mar 18;12(3):4. doi: 10.1055/a-2282-6123. eCollection 2024 Mar. Endosc Int Open. 2024. PMID: 38504748 Free PMC article.
Abstract
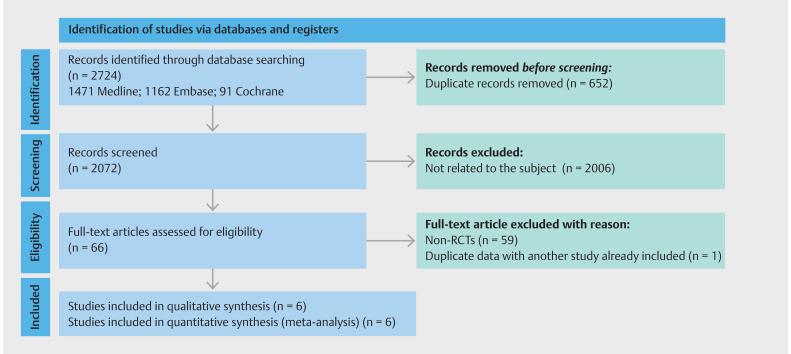
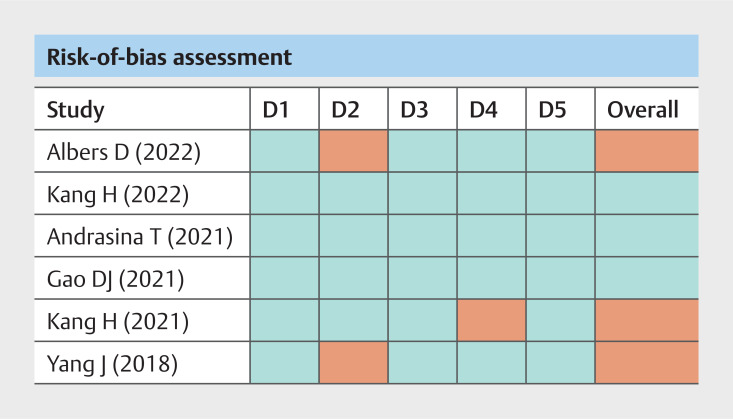
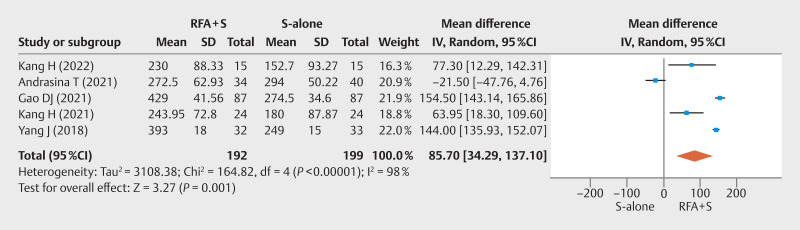
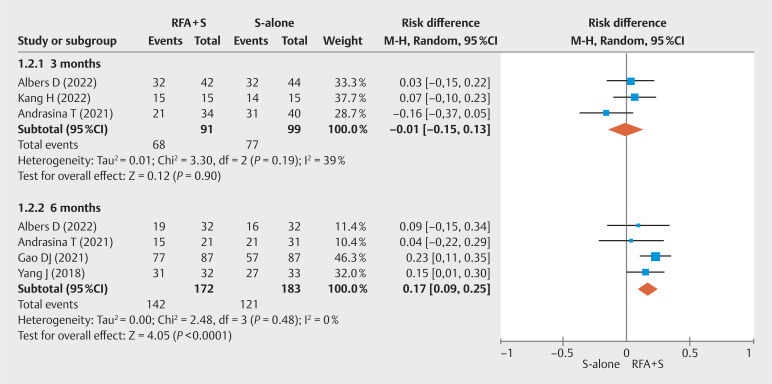
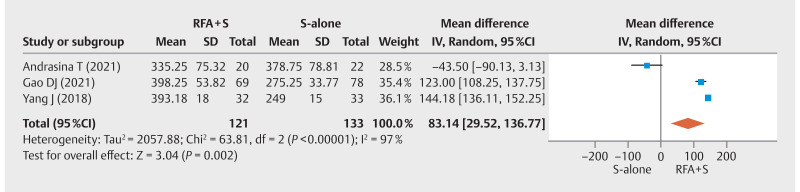
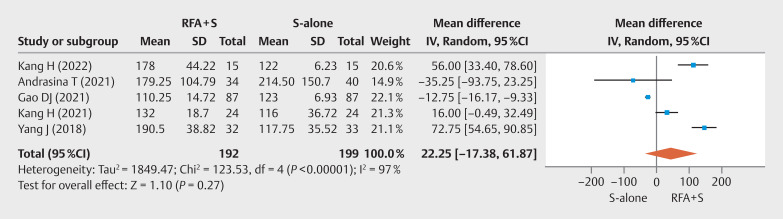
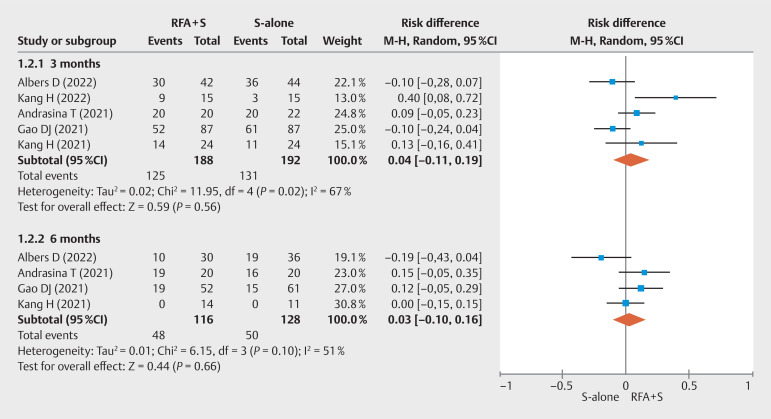
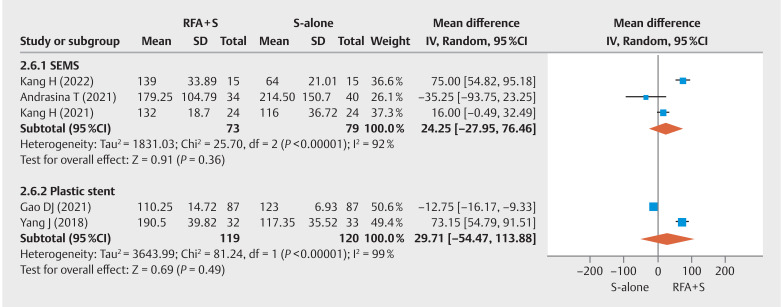
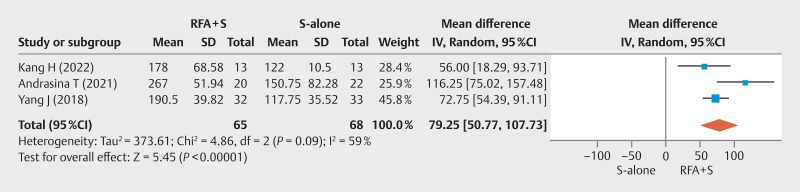
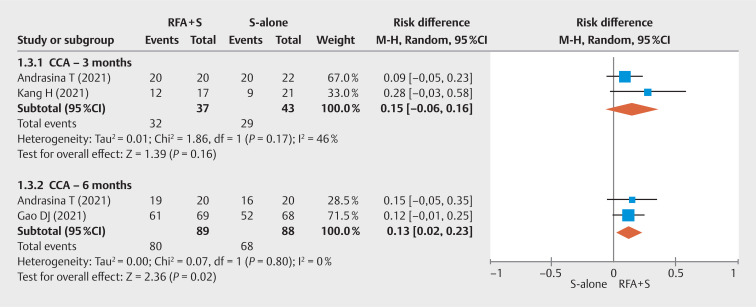
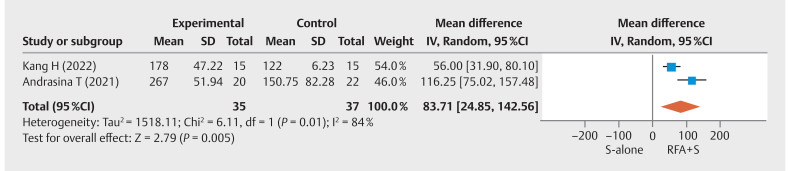
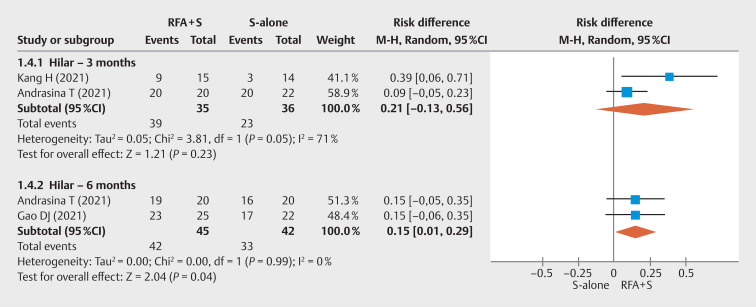
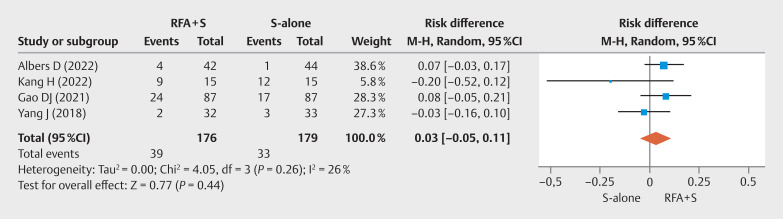
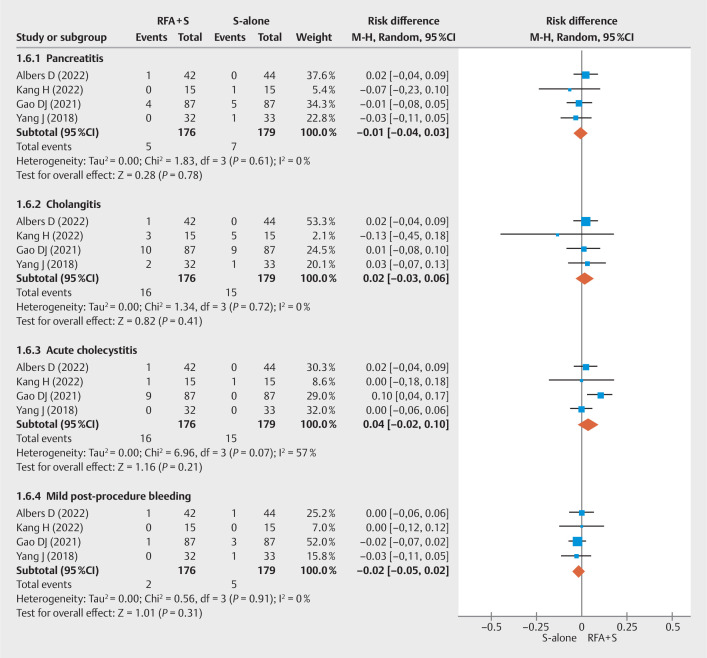
Background and study aims Recurrent biliary stent occlusion and tumor ingrowth remain a major concern among patients with malignant biliary obstruction (MBO) with significant impact on patient morbidity and survival. Intraductal radiofrequency ablation (RFA) has emerged as a promising treatment that seeks to extend stent patency. This study aimed to evaluate the impact of RFA on overall survival (OS) and stent patency among patients with unresectable MBO. Methods A comprehensive search of electronic databases was performed for randomized controlled trials (RCTs) comparing RFA plus biliary stent (RFA+S) versus biliary stent alone (S-alone). Outcomes assessed included overall survival, stent patency, and adverse events (AEs) with mean difference (MD) calculated from pooled proportions. Subgroup analyses were performed for hilar strictures and cholangiocarcinoma (CCA). Results Six RCTs (n=439 patients) were included and demonstrated improved survival among patients who received RFA+S (MD 85.80 days; 95% confidence interval [CI] 35.02-136.58; I 2 =97%; P <0.0009). The pooled MD for total stent patency was 22.25 days (95% CI 17.38-61.87; I 2 =97%; P =0.27). There was no difference in AEs between RFA+S vs S-alone ( P >0.05). On subgroup analyses, RFA+S was associated with improved stent patency (MD 76.73 days; 95% CI 50.11-103.34; I 2 =67%; P <0.01) and OS (MD 83.14 (95% CI 29.52-136.77; I 2 =97%; P <0.01] for CCA. For hilar strictures, stent patency was improved among patients with RFA+S [MD 83.71 days (95% CI 24.85-142.56; I 2 =84%; P <0.01]. Conclusions RFA+S improved OS in the treatment of MBO when compared with S-alone. Moreover, the RFA therapy prolonged stent patency in hilar strictures and CCA, with similar rates of AEs.
Keywords: PTCD/PTCS; Strictures.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Conflict of Interest Dr. Diogo Turiani Hourneaux De Moura: BariaTek Medical - Advisory Board Member (Consulting fees). This was not relevant to this study. Dr. Eduardo Guimaraes Hourneaux De Moura: Olympus - Consultant (Consulting fees) and Boston Scientific - Consultant (Consulting fees). These were not relevant to this study. The other authors declare no potential conflict of interest.
Figures
Similar articles
-
Survival Benefit of Intraductal Radiofrequency Ablation for Malignant Biliary Obstruction: A Systematic Review with Meta-Analysis.Clin Endosc. 2021 Jan;54(1):100-106. doi: 10.5946/ce.2020.254. Epub 2021 Jan 15. Clin Endosc. 2021. PMID: 33445841 Free PMC article.
-
Adjuvant Radiofrequency Ablation Along With Stenting Versus Stenting Alone for Biliary Tree Drainage in Patients With Malignant Biliary Strictures: A Systemic Review and Meta-analysis.J Clin Gastroenterol. 2024 Mar 1;58(3):297-306. doi: 10.1097/MCG.0000000000001851. J Clin Gastroenterol. 2024. PMID: 37039475
-
Local palliative therapies for unresectable malignant biliary obstruction: radiofrequency ablation combined with stent or biliary stent alone? An updated meta-analysis of nineteen trials.Surg Endosc. 2022 Aug;36(8):5559-5570. doi: 10.1007/s00464-022-09181-2. Epub 2022 Mar 16. Surg Endosc. 2022. PMID: 35296949 Review.
-
Effect of radiofrequency ablation in addition to biliary stent on overall survival and stent patency in malignant biliary obstruction: an updated systematic review and meta-analysis.Eur J Gastroenterol Hepatol. 2023 Jun 1;35(6):646-653. doi: 10.1097/MEG.0000000000002568. Epub 2023 Apr 25. Eur J Gastroenterol Hepatol. 2023. PMID: 37129575
-
Impact of temperature-controlled endobiliary radiofrequency ablation for inoperable hilar cholangiocarcinoma: A propensity score-matched analysis.Endosc Int Open. 2024 Apr 15;12(4):E535-E544. doi: 10.1055/a-2276-1897. eCollection 2024 Apr. Endosc Int Open. 2024. PMID: 38720905 Free PMC article.
Cited by
-
Perspectives on biliary radiofrequency ablation: Review of a recent meta-analysis.Endosc Int Open. 2024 May 3;12(5):E639. doi: 10.1055/a-2289-9788. eCollection 2024 May. Endosc Int Open. 2024. PMID: 38707597 Free PMC article. No abstract available.
-
Biliary stents for active materials and surface modification: Recent advances and future perspectives.Bioact Mater. 2024 Sep 13;42:587-612. doi: 10.1016/j.bioactmat.2024.08.031. eCollection 2024 Dec. Bioact Mater. 2024. PMID: 39314863 Free PMC article. Review.
-
Reply to Chandrasekhara and Aggarwal.Endosc Int Open. 2024 May 3;12(5):E640-E641. doi: 10.1055/a-2295-3143. eCollection 2024 May. Endosc Int Open. 2024. PMID: 38707598 Free PMC article. No abstract available.
-
Endoscopic treatment of unresectable perihilar cholangiocarcinoma: beyond biliary drainage.Therap Adv Gastroenterol. 2025 Apr 14;18:17562848251328595. doi: 10.1177/17562848251328595. eCollection 2025. Therap Adv Gastroenterol. 2025. PMID: 40292090 Free PMC article. Review.
-
The effect of percutaneous endobiliary radiofrequency ablation on biliary stent patency.Sci Prog. 2025 Apr-Jun;108(2):368504251356422. doi: 10.1177/00368504251356422. Epub 2025 Jun 30. Sci Prog. 2025. PMID: 40586160 Free PMC article.
References
-
- Adler D, Byrne K. Endoscopic stenting for malignant biliary obstruction. Post TW, ed UpToDate Waltham, MA: UpToDate Inc. https://www.uptodate.com https://www.uptodate.com
-
- Chandrasekar VT, Faigel D. Diagnosis and treatment of biliary malignancies: biopsy, cytology, cholangioscopy and stenting. Mini-invasive Surgery. 2021 doi: 10.20517/2574-1225.2021.12. - DOI
Publication types
LinkOut - more resources
Full Text Sources