

Bilateral carotid dissection due to Eagle syndrome
- PMID: 38188950
- PMCID: PMC10767265
- DOI: 10.1016/j.radcr.2023.11.028
Bilateral carotid dissection due to Eagle syndrome
Abstract
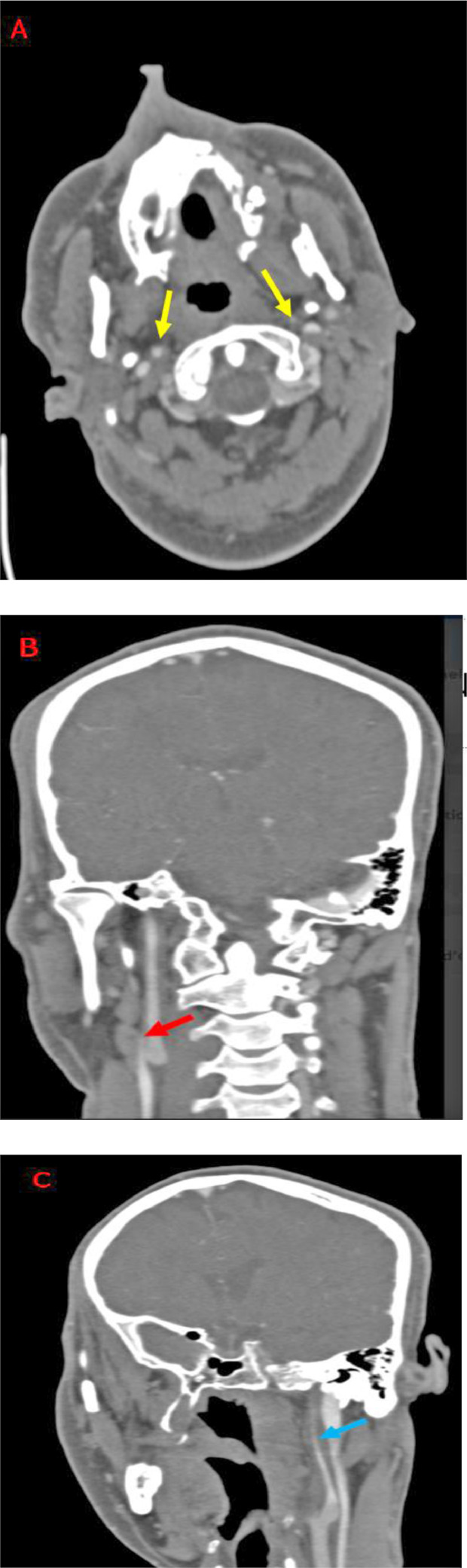
Eagle syndrome is defined as a collection of symptoms affecting the cervical and cranial regions, resulting from an elongated styloid process or ossified stylohyoid ligament encroaching on surrounding structures and causing a variety of symptoms. Classically, Eagle syndrome presents as neck, throat, or ear pain. Carotid artery dissection is a rare complication of Eagle syndrome. We report the case of a 40-year-old man who presented with bilateral internal carotid artery dissection secondary to pathological elongation of the styloid processes.
Keywords: Carotid dissection; Eagle syndrome; Elongated styloid process.
© 2023 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures



References
-
- Eagle WW. Elongated styloid processes: report of two cases. Arch Otolaryngol. 1937;25:584–587.
-
- Eagle WW. Elongated styloid process; further observations and a new syndrome. Arch Otolaryngol. 1948;47:630–640. - PubMed
-
- Gozil R, Yener N, Calguner E, Araç M, Tunç E, et al. Morphological characteristics of styloid process evaluated by computerized axial tomography. Ann Anat. 2001;183:527–535. - PubMed
-
- Okabe S, Morimoto Y, Ansai T, et al. Clinical significance and variation of the advanced calcified stylohyoid complex detected by panoramic radiographs among 80-year-old subjects. Dentomaxillofac Radiol. 2006;35:191–199. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
