

A simple and efficient clinical prediction scoring system to identify malignant pleural effusion
- PMID: 38189181
- PMCID: PMC10775726
- DOI: 10.1177/17534666231223002
A simple and efficient clinical prediction scoring system to identify malignant pleural effusion
Abstract
Background: Early diagnosis of malignant pleural effusion (MPE) is of great significance. Current prediction models are not simple enough to be widely used in heavy clinical work.
Objectives: We aimed to develop a simple and efficient clinical prediction scoring system to distinguish MPE from benign pleural effusion (BPE).
Design: This retrospective study involved patients with MPE or BPE who were admitted in West China Hospital from December 2010 to September 2016.
Methods: Patients were divided into training, testing, and validation set. Prediction model was developed from training set and modified to a scoring system. The diagnostic efficacy and clinical benefits of the scoring system were estimated in all three sets.
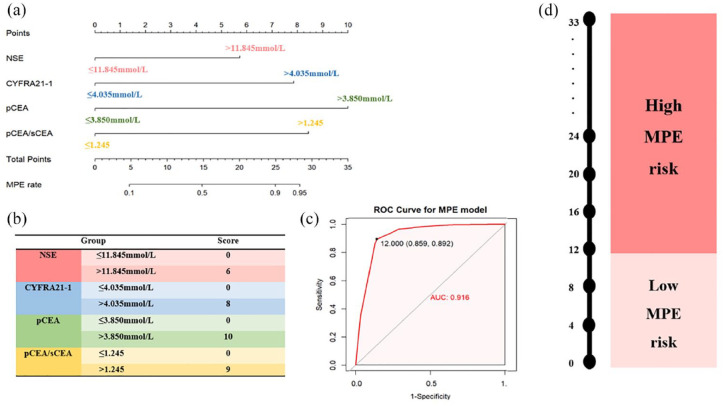
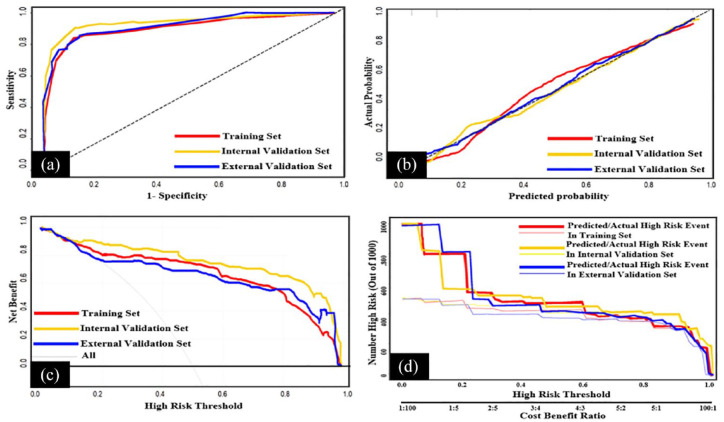
Results: Finally, 598 cases of MPE and 1094 cases of BPE were included. Serum neuron-specific enolase, serum cytokeratin 19 fragment (CYFRA21-1), pleural carcinoembryonic antigen (CEA), and ratio of pleural CEA to serum CEA were selected to establish the prediction models in training set, which were modified to the scoring system with scores of 6, 8, 10, and 9 points, respectively. Patients with scores >12 points have high MPE risk while ⩽12 points have low MPE risk. The scoring system has a high predictive value and good clinical benefits to differentiate MPE from BPE or lung-specific MPE from BPE.
Conclusion: This study developed a simple clinical prediction scoring system and was proven to have good clinical benefits, and it may help clinicians to separate MPE from BPE.
Keywords: clinical prediction model; diagnosis; malignant pleural effusion; scoring system.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures

Similar articles
-
Diagnostic Value of Six Tumor Markers for Malignant Pleural Effusion in 1,230 Patients: A Single-Center Retrospective Study.Pathol Oncol Res. 2022 Apr 20;28:1610280. doi: 10.3389/pore.2022.1610280. eCollection 2022. Pathol Oncol Res. 2022. PMID: 35515016 Free PMC article.
-
Development and validation of a novel scoring system developed from a nomogram to identify malignant pleural effusion.EBioMedicine. 2020 Aug;58:102924. doi: 10.1016/j.ebiom.2020.102924. Epub 2020 Jul 30. EBioMedicine. 2020. PMID: 32739872 Free PMC article. Clinical Trial.
-
Development and Validation of a Scoring System for Early Diagnosis of Malignant Pleural Effusion Based on a Nomogram.Front Oncol. 2021 Dec 7;11:775079. doi: 10.3389/fonc.2021.775079. eCollection 2021. Front Oncol. 2021. PMID: 34950585 Free PMC article.
-
Evaluation of predictive value of pleural CEA in patients with pleural effusions and histological findings: A prospective study and literature review.Clin Biochem. 2016 Nov;49(16-17):1227-1231. doi: 10.1016/j.clinbiochem.2016.08.006. Epub 2016 Aug 10. Clin Biochem. 2016. PMID: 27521620 Review.
-
Diagnostic value of carcinoembryonic antigen in malignant pleural effusion: a meta-analysis.Respirology. 2008 Jun;13(4):518-27. doi: 10.1111/j.1440-1843.2008.01291.x. Epub 2008 Apr 14. Respirology. 2008. PMID: 18422869
Cited by
-
Predictive model for sarcopenia in patients with non-small cell lung cancer and malignant pleural effusion.BMC Cancer. 2025 Feb 25;25(1):350. doi: 10.1186/s12885-025-13772-2. BMC Cancer. 2025. PMID: 40000963 Free PMC article.
-
Development and validation of a prediction model based on a nomogram for tuberculous pleural effusion.Front Med (Lausanne). 2025 Jul 18;12:1589406. doi: 10.3389/fmed.2025.1589406. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40757203 Free PMC article.
References
-
- Wang G, Wang S, Yang X, et al. Accuracy of Xpert MTB/RIF ultra for the diagnosis of pleural TB in a multicenter cohort study. Chest 2020; 157: 268–275. - PubMed
-
- Porcel JM, Gasol A, Bielsa S, et al. Clinical features and survival of lung cancer patients with pleural effusions. Respirology 2015; 20: 654–659. - PubMed
-
- Fortin M, Taghizadeh N, Tremblay A. Procedures performed during hospitalizations for malignant pleural effusions: data from the 2012 National Inpatient Sample. Respiration 2018; 95: 228–234. - PubMed
-
- Kassirian S, Hinton SN, Cuninghame S, et al. Diagnostic sensitivity of pleural fluid cytology in malignant pleural effusions: systematic review and meta-analysis. Thorax 2023; 78: 32–40. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
