

The overlap of chronic obstructive pulmonary disease and obstructive sleep apnea in hospitalizations for acute exacerbation of chronic obstructive pulmonary disease
- PMID: 38189375
- PMCID: PMC11145048
- DOI: 10.5664/jcsm.11000
The overlap of chronic obstructive pulmonary disease and obstructive sleep apnea in hospitalizations for acute exacerbation of chronic obstructive pulmonary disease
Abstract
Study objectives: This study examined in-hospital outcomes for patients with both chronic obstructive pulmonary disease (COPD) and obstructive sleep apnea (OSA), also known as COPD-OSA overlap syndrome, during hospitalizations for acute exacerbation of COPD.
Methods: The National Inpatient Sample was used to examine in-hospital mortality, length of stay, costs, and utilization of supportive ventilation in patients with COPD-OSA overlap during acute exacerbation of COPD hospitalizations. A 1-to-1 matched case-control design was utilized to match patients with and without OSA. Multivariate logistic regression modeling was used to examine mortality and ventilatory support, while controlling for potentially confounding diagnoses.
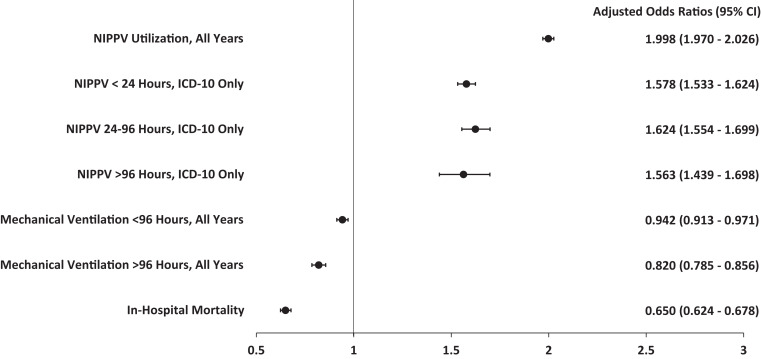
Results: COPD-OSA overlap was associated with longer median length of stay (4 days OSA, 3 days non-OSA; P < .001), higher mean costs ($32,197 OSA, $29,011 non-OSA; P < .001), increased utilization of noninvasive positive-pressure ventilation (13.92% OSA, 6.78% non-OSA; P < .001), and when required for greater than 96 hours, earlier initiation of mechanical ventilation (2.53 days OSA, 3.35 days non-OSA; P = .001). However, COPD-OSA overlap was associated with reduced mortality (0.81% OSA, 1.05% non-OSA; P < .001). These differences in mortality (adjusted odds ratio: 0.650; 95% confidence interval: 0.624-0.678) and noninvasive positive-pressure ventilation usage (adjusted odds ratio: 1.998; 95% confidence interval: 1.970-2.026) remained when adjusted for confounders.
Conclusions: Patients with COPD-OSA overlap have higher utilization of supportive ventilation and longer length of stay during acute exacerbation of COPD hospitalizations, contributing to higher costs. The diagnosis of OSA is associated with reduced mortality in these hospitalizations, which may be related to greater utilization of supportive ventilation when OSA is recognized.
Citation: De la Fuente JRO, Greenberg P, Sunderram J. The overlap of chronic obstructive pulmonary disease and obstructive sleep apnea in hospitalizations for acute exacerbation of chronic obstructive pulmonary disease. J Clin Sleep Med. 2024;20(6):863-870.
Keywords: COPD; COPD exacerbations; OSA; inpatient outcomes; overlap syndrome.
© 2024 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have reviewed and approved this manuscript. Work for this study was performed at Rutgers Robert Wood Johnson Medical School. The authors report no conflicts of interest.
Figures

References
-
- Diaz-Guzman E , Mannino DM . Epidemiology and prevalence of chronic obstructive pulmonary disease . Clin Chest Med. 2014. ; 35 ( 1 ): 7 – 16 . - PubMed
-
- Adeloye D , Song P , Zhu Y , Campbell H , Sheikh A , Rudan I ; NIHR RESPIRE Global Respiratory Health Unit . Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis . Lancet Respir Med. 2022. ; 10 ( 5 ): 447 – 458 . - PMC - PubMed
-
- Senaratna CV , Perret JL , Lodge CJ , et al. . Prevalence of obstructive sleep apnea in the general population: a systematic review . Sleep Med Rev. 2017. ; 34 : 70 – 81 . - PubMed
-
- Drager LF , McEvoy RD , Barbe F , Lorenzi-Filho G , Redline S ; INCOSACT Initiative (International Collaboration of Sleep Apnea Cardiovascular Trialists) . Sleep apnea and cardiovascular disease: lessons from recent trials and need for team science . Circulation. 2017. ; 136 ( 19 ): 1840 – 1850 . - PMC - PubMed
-
- Trzepizur W , Blanchard M , Ganem T , et al. . Sleep apnea—specific hypoxic burden, symptom subtypes, and risk of cardiovascular events and all-cause mortality . Am J Respir Crit Care Med. 2022. ; 205 ( 1 ): 108 – 117 . - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
